
3-Dimensional Visualization of Impacted Maxillary CuspidsJames Mah, DDS, MSc, MRCD, DMSc
Assistant Professor, USC School of Dentistry Director of the Craniofacial Virtual Reality Laboratory (cvrl.usc.edu) From the Winter 2003 AADMRT Newsletter  Dr. James Mah Dr. James Mah
Visualization of impacted maxillary cuspids is essential to their treatment planning and determination of prognosis. Current methods generally utilize multiple views, typically a panoramic view supplemented with an occlusal view. However, these methods can be limited in their ability to accurately identify a tooth's position and to reveal essential anatomy related to the impacted tooth such as an eruption cyst and extent of resorption/displacement of adjacent teeth (Figure 1 — Panoramic showing bilateral impacted maxillary cuspids with resorption of the lateral incisors). 3-dimensional volumetric imaging can resolve many of the shortcomings of traditional methods, particularly those associated with projection and perspective and allow for more accurate viewing and determination of the impacted tooth's position. Therefore, in this report we will describe and discuss the utilization of 3-dimensional volumetric imaging (NewTom 9000, Aperio Services) in the visualization of maxillary impacted cuspids.

Figure 1: Panoramic of Bilateral Impacted Cuspids with Resorption of Lateral Incisors.
|






|
Volumetric imaging devices developed specifically for dentistry are a relatively recent occurrence. The NewTom 9000 is the first and is still the only available device (Figure 2 NewTom 9000 Volumetric Imaging Device for Dentistry). In contrast to the fanshaped beam of medical CT devices, it features a cone-beam radiation path providing a series of images as the x-ray tube makes one 360 degree-rotation about the patient. The device provides a 13 cm vertical field of view, large enough to contain the maxilla and mandible without cranial base structures (Figure 3 — NewTom volume with full opacity to illustrate the field of view). The accompanying software constructs a volume that can be viewed from multiple perspectives using secondary reconstruction tools to create axial, transaxial, panoramic and other views (Figure 4a — Reconstructed panoramic view; Figure 4b: Reconstructed Frontal, occlusal and lateral transaxials). Export features in DICOM or BMP format allows for viewing using common volume rendering programs (Figure 5 — Volume of same patient as Figure4 viewed in VolviewTM).

Figure 2: NewTom 9000 Volumetric Imaging Device for Dentistry
|
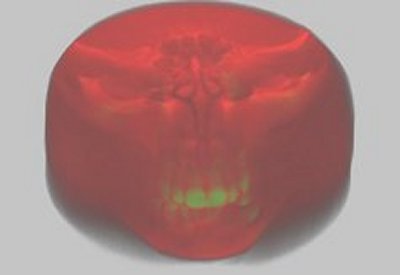
Figure 3: NewTom volume with full opacity to illustrate the field of view.
|

Figure 4a: Reconstructed Panoramic View.
The maxillary cuspid is the most commonly impacted tooth, second only to third molars. This is not surprising considering its eruptive path and sequences of dental eruption. The maxillary cuspid forms in its developmental crypt in close proximity to the infraorbital rim. From this position it erupts into occlusion, over a period of years, following a circuitous "S" path during which many events can occur which lead to its impaction. Additionally, the maxillary cuspid typically erupts following the first premolar and at the same time or following the second premolar. With these sequences, insufficient arch length can greatly increase the chance of impaction. The earlier erupting premolars simply occupy and limit space to accommodate the cuspid into the dental arch.
Clinicians should suspect that a cuspid is impacted when there is delayed eruption, asymmetry, small/peg/missing lateral incisors, space loss in the area, severe arch length deficiency or a family history of cuspid impaction. Once an impacted cuspid is suspected, the role of imaging is to confirm this condition as opposed to a delay in eruption or congenital absence of the tooth. Secondly, imaging will play a fundamental role in the management of the impacted cuspid by the orthodontist and the surgeon who will uncover the tooth.
Clinicians should suspect that a cuspid is impacted when there is delayed eruption, asymmetry, small/peg/missing lateral incisors, space loss in the area, severe arch length deficiency or a family history of cuspid impaction. Once an impacted cuspid is suspected, the role of imaging is to confirm this condition as opposed to a delay in eruption or congenital absence of the tooth. Secondly, imaging will play a fundamental role in the management of the impacted cuspid by the orthodontist and the surgeon who will uncover the tooth.

|

|
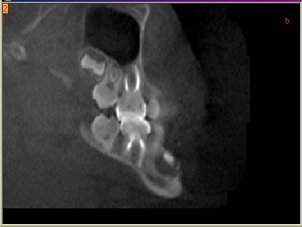
Figure 4b: Reconstructed Fronal, Occlusal and Lateral Views.
Traditional approaches to localizing impacted maxillary cuspids essentially apply image-tube shift principles (reviewed by Jacobs, 1999). More reliable approaches use a panoramic with an occlusal view taken with a slight vertical shift (70-75 degrees from horizontal compared to the traditional 60-65 degrees). Less reliable methods involve image magnification compared to the normal contralateral tooth and image superimposition on the central and lateral incisor. Without a good idea of the impacted cuspid location, surgeons must create larger access openings to expose the crown and will sound multiple possible tooth locations by perforating through the bony cortex with an instrument or a periodontal probe to feel for the tooth. A good understanding of the impacted tooth's position will also assist the orthodontist in designing biomechanics to best move the tooth . It is clear that 3- D volumetric imaging provides added clinical value to imaging, allowing for more efficient and less invasive surgery as well as better designs of biomechanics to upright and align the impacted tooth.
|
Volumetric imaging of impacted maxillary cuspids is providing new insights into their location, features and impact on adjacent teeth. In a study of 107 children, Ericson and Kurol, 2000 found that 93% of ectopic canines in contact with the roots of the lateral incisor (as opposed to 49% of normally erupting canines) and 19% in contact with the central incisor.
|
|
Root resorption on incisor roots adjacent to ectopically positioned canine occurred in 38% of the laterals and in 9% of the centrals. This research group also found that dental follicles of ectopically erupting canines were, on average, wider than those of the normally erupting canines (Ericson and Bjerklin, 2001).
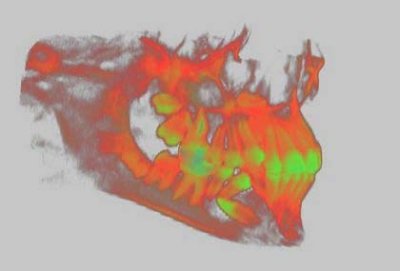
Figure 5: Same volume as Figure 4 viewed with VolviewTM volume rendering software.
While the above research was conducted using medical CT devices, a concern with their use for "routine" dental examination is the risk worth the benefit. Radiation dosimetry studies conducted by our research group have placed the effective dose absorbed during a maxillo-facial examination with the NewTom 9000 at 50.3 microSieverts (µSv). For purposes of comparison, a panoramic radiograph is in the range of 2.9 — 9.6 µSv, a full mouth series ranges from 33 to 84 µSv (reviewed in Danforth and Clark) and conventional CT imaging of a region of the maxilla ranges from 17.6 - 656.9 µSv and the mandible ranges from 124.9 - 250.3 µSv. Bear in mind the NewTom volume includes both the maxilla and the mandible at 50.3 µSv. Given these data, the risk:benefit for a NewTom imaging session for dental applications is justified in the context of currently available imaging modalities.
In summary, 3-D volumetric imaging provides essential information for clinicians to better manage impacted maxillary cuspids. A good understanding of the tooth's position and its relationship to adjacent teeth and structures greatly facilitates clinical decisions. In addition, this approach is revealing new information on impacted cuspids. Similar benefits are being found in management of other impacted teeth. With these benefits, 3-D volumetric imaging has great potential in future of dental care.
In summary, 3-D volumetric imaging provides essential information for clinicians to better manage impacted maxillary cuspids. A good understanding of the tooth's position and its relationship to adjacent teeth and structures greatly facilitates clinical decisions. In addition, this approach is revealing new information on impacted cuspids. Similar benefits are being found in management of other impacted teeth. With these benefits, 3-D volumetric imaging has great potential in future of dental care.
References
Danforth RA, Clark DE. Effective dose from radiation absorbed during a panoramic examination with a new generation machine. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000:89(2);236-43
Ericson S, Bjerklin K. The dental follicle in normally and ectopically erupting maxillary canines: a CT study. Angle Orthod 2001:71(5);333-42
Ericson S. Kurol PJ. Resorption of incisors after ectopic eruption of maxillary canines: a CT study Angle Orthod 2000:70(6);415-23
Jacobs SG. Localization of the unerupted maxillary canine: How to and when to. Am J Orthod Dentofac Orthop 1999:115(3);314-22
Ericson S, Bjerklin K. The dental follicle in normally and ectopically erupting maxillary canines: a CT study. Angle Orthod 2001:71(5);333-42
Ericson S. Kurol PJ. Resorption of incisors after ectopic eruption of maxillary canines: a CT study Angle Orthod 2000:70(6);415-23
Jacobs SG. Localization of the unerupted maxillary canine: How to and when to. Am J Orthod Dentofac Orthop 1999:115(3);314-22