
CBCT Imaging in Private Practice
Scott A. Smith, D.D.S.
Practice Limited to Periodontics and Dental Implants Merced and Turlock, California From the Summer 2011 AADMRT Newsletter  Scott A. Smith, DDS Scott A. Smith, DDS
As a Periodontist in private practice for 22 years, I have traditionally used 2-dimensional (2-D) radiographic images (i.e., bitewing, periapical and panoramic) to diagnose and treat my patients. A large percentage of my practice is limited to the treatment of periodontal (gum) disease where I still continue to rely on this very reliable form of radiographic imaging.
Another large percentage of my private practice includes the surgical placement of dental implants. It is this aspect of my practice where the reliability of 2-D radiographic images is often times insufficient. I do continue to utilize 2-D films for implants, but usually as a "reference" as I will expound on later. I wish to take you through the steps I use in my implant practice for the utilization of CBCT. From a surgical perspective, it is of the utmost importance to protect vital anatomic structures from the trauma of surgery. When surgically placing dental implants, whether it is in the maxilla or the mandible, one simply cannot rely solely upon 2-D imaging. PATIENT CONSULTATION
As is often the routine on my practice, patients will either refer themselves to my office for an implant consultation, or their General Dentist will refer them to my office. Some patients require the treatment and management of their periodontal disease, but for the purpose of this article I will limit my comments on the implant patient referral. The majority of the patients I see, often times walk into my practice with a 2-D pano in their hands as that is the most common film acquired in the general dental office. Most of the patients I see are partially edentulous (missing some but not all teeth) but a few present completely edentulous. Since the panoramic film has a much larger image discrepancy, I will often take periapical films of the edentulous sites. This is my "reference," if you will, for a general view of anatomic structures, such as sinus and nerve proximity. Some measurements with implant overlays can be used for general implant planning. The cost to administer this to the patient is low and, if patients do not commit to implant treatment, for whatever reason, they have incurred only a small cost for our consultation. |






|

Fig. 1: Clinical intraoral partially edentulous tooth #18 and 19
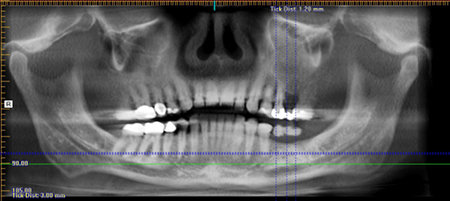
Fig. 2: Panoramic view from iCat Vision. Radiographic barium guide in place to simulate tooth position #18 and 19
CBCT SCAN
Once the decision is made by the patient to move forward with implants we will order our CBCT from our imaging center. Depending on the size of the edentulous space, we will fabricate a barium sulfate guide to simulate the missing teeth, which the patient will take to their scanning appointment. With the implant treatment planning software we utilize in our practice (Simplant by Materialise), we can often order our scan without the barium guide. This is accomplished by placing virtual teeth within the software treatment plan, allowing virtual placement of the dental implant in relation to the appropriate prosthetic requirements.
After our patients our scanned, we receive a packet from the scanning facility. Within that packet, we receive intraoral photos of the patient, all raw dicom files and a disk allowing us to utilized iCat Vision software. This is very helpful as its viewer is installed on any computer allowing myself, and/or my referring GP's to view the patient scan. In addition, we also receive a very nice printout of the volumetric scans of the particular implant site.
As iCat Vision does not allow for implant treatment planning or surgical guide fabrication, we will submit the provided raw dicom files for conversion to Simplant. Once converted, I can then plan the entire case on the computer, sit with my referring GP, manipulate implants within the bone, choose proper abutments and see the final case on the computer before any surgery. If the scan shows inadequate volume of bone, in relation to the proper dental implant location, then I can plan for bone augmentation surgery in order to provide adequate bone volume as dictated by the software. With either iCat vision or Simplant, we can sit with the patient, as well, and review his or her own personal case with them. This truly personalizes their treatment.
Once the decision is made by the patient to move forward with implants we will order our CBCT from our imaging center. Depending on the size of the edentulous space, we will fabricate a barium sulfate guide to simulate the missing teeth, which the patient will take to their scanning appointment. With the implant treatment planning software we utilize in our practice (Simplant by Materialise), we can often order our scan without the barium guide. This is accomplished by placing virtual teeth within the software treatment plan, allowing virtual placement of the dental implant in relation to the appropriate prosthetic requirements.
After our patients our scanned, we receive a packet from the scanning facility. Within that packet, we receive intraoral photos of the patient, all raw dicom files and a disk allowing us to utilized iCat Vision software. This is very helpful as its viewer is installed on any computer allowing myself, and/or my referring GP's to view the patient scan. In addition, we also receive a very nice printout of the volumetric scans of the particular implant site.
As iCat Vision does not allow for implant treatment planning or surgical guide fabrication, we will submit the provided raw dicom files for conversion to Simplant. Once converted, I can then plan the entire case on the computer, sit with my referring GP, manipulate implants within the bone, choose proper abutments and see the final case on the computer before any surgery. If the scan shows inadequate volume of bone, in relation to the proper dental implant location, then I can plan for bone augmentation surgery in order to provide adequate bone volume as dictated by the software. With either iCat vision or Simplant, we can sit with the patient, as well, and review his or her own personal case with them. This truly personalizes their treatment.
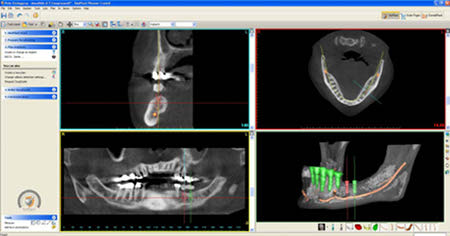
Fig. 3: Simplant software conversion: x-section, axial, panoramic and 3D orientation
SURGICAL GUIDE
In order to precisely place the dental implants, we will often order a surgical guide. The Simplant software has this feature built into it. After completing the planning phase within the software, the information is uploaded and a surgical guide is fabricated and milled allowing directional control, depth control, or both. The majority of our cases utilize this feature. Only when I immediately place a dental implant following same day extraction will I not use a guide simply because the extraction socket allows me complete clinical insight for proper implant placement.
In order to precisely place the dental implants, we will often order a surgical guide. The Simplant software has this feature built into it. After completing the planning phase within the software, the information is uploaded and a surgical guide is fabricated and milled allowing directional control, depth control, or both. The majority of our cases utilize this feature. Only when I immediately place a dental implant following same day extraction will I not use a guide simply because the extraction socket allows me complete clinical insight for proper implant placement.

Fig. 4: Surgical guide
|

Fig. 5: Surgical guide intraoral
|

Fig. 6: Final restorations. Implant crowns #18 and 19. Crown tooth #20
CONCLUSION
There is definitely a place for CBCT in the clinical practice and for computer-guided implant surgery. In areas where vital anatomic structures are at risk of trauma, this treatment modality affords clinician's greater confidence and patients a higher level of safety. In our practice there really is no margin for error and with the technology of CBCT we can potentially eliminate error.
There is definitely a place for CBCT in the clinical practice and for computer-guided implant surgery. In areas where vital anatomic structures are at risk of trauma, this treatment modality affords clinician's greater confidence and patients a higher level of safety. In our practice there really is no margin for error and with the technology of CBCT we can potentially eliminate error.