
CBCT: Savior or Devil?Timothy Mickiewicz, D.D.S.
Private practice, Sacramento, California Specialist in Oral Facial Pain, TMD and Sleep Medicine From the Spring 2011 AADMRT Newsletter  Timothy Mickiewicz, DDS Timothy Mickiewicz, DDS
Dentists traditionally practice in a bubble. Lacking the collegiality of large medical groups, hospitals or multi-specialty dental clinics, we are often left to fend for ourselves when faced with complex medico-dental issues. True we have developed a model of having a stable of specialists for referral and consult, more often though, generalists are choosing to do more complex specialty procedures. Much of this may be driven by our individualist nature, my gut tells me much is driven by economics. The vast majority of generalists are a dedicated, well intentioned lot. Continuing education is more advanced and the days of signing in at a resort to watch a video presentation with simultaneous development of your fabulous tan are pretty much over. The resulting realization by general dentists and specialists alike is the actualization of the more I know...the more I know how much I don't know phenomenon. Educators are hard pressed to cram enough information into the average dental student just to make them a "safe beginner." There are few opportunities for an apprentice situation with experienced dentists and the debt load of the recent grads is onerous. Experienced dentists can become continuing education junkies, running from one dental guru to the next in search of new skill sets. Increasing their knowledge base and looking for profit centers can lead to a serious concern regarding the standards of care. Tools are available, information readily accessible through the internet, and every dental magazine is filled with ads and advertorials touting the latest gadget to make your profits soar. Dentists love gadgets.
Recently, the New York Times ran a prominent piece regarding the relative explosion of CBCT and increased radiation exposure. While not a true hit piece on the procedure, relevant questions were raised, links to sponsored speakers were questioned and my sense was that the "gee whiz" factor and profit being the motivation behind this advanced technology is the real problem in their opinion. (The flipside was presented and I can't believe there are dentists who still use D speed film!) This brings us back to the controversial standard of care issue and the ability to adjust your opinion based upon how much you embrace this amazing technology. There were also some interesting stats presented that were likely over the head of the lay reader. Comparing a conventional CT head scan vs. CBCT vs. Panoramic imaging. Basically, conventional CT equals 125 panoramics... CBCT 4-5. Given the amount of information obtained, the quality of imaging, and the ability to interpret relevant information that could make or break an implant or orthognathic case, I strongly favor the CBCT. |





|
Over the past 20 years I have developed one of the largest orofacial pain and sleep medicine practices in Northern California. I made CBCT part of my standard of care as our practice is often the place of last resort for many patients. The practice base is primarily physician referral and consequently I am blessed with access to some of the great minds representing the medical specialties. This unique melding of medicine and dentistry is my personal goal for the model of dentistry. It would be unachievable without the cooperation of my colleagues and access to the latest diagnostic tools. I have witnessed the evolution and revolution of imaging capabilities and frankly I question how we can practice without using every tool in our arsenal. So many times I have been fooled by what I consider to be an excellent digital panoramic we use to screen patients only to find major degenerative joint changes on CBCT. I realize that my practice is unique and the expense of digital imaging can be daunting. I feel however that without it I am a lesser dentist. I readily admit to the humbling experience of checking margins blown up to reveal unacceptable integrity...I also have the integrity to replace that crown at my expense.
Diagnostically it is really quite simple:
Various organizations refuse to fully embrace the widespread use of CBCT. Some manufacturers have helped foster this by having machines that are programmed to only see limited troughs i.e.; for implant placement. The diagnosis of degenerative joints prior to orthodontics or major restorative treatment is critical. Nothing is more frustrating for a patient, parent and dentist as having a major occlusal asymmetry suddenly appearing prior to debanding an orthodontic case. Pretreatment diagnosis would save many of these cases and keep the attorneys at bay.
Diagnostically it is really quite simple:
- Our ears...listen to the patient to make an accurate diagnosis
- Our brains...being a constant student and thinking outside of the box
- Our technology...confirm the diagnosis with the appropriate tools
- Our obligation to the patient...learn from each case so the next patient benefits
Various organizations refuse to fully embrace the widespread use of CBCT. Some manufacturers have helped foster this by having machines that are programmed to only see limited troughs i.e.; for implant placement. The diagnosis of degenerative joints prior to orthodontics or major restorative treatment is critical. Nothing is more frustrating for a patient, parent and dentist as having a major occlusal asymmetry suddenly appearing prior to debanding an orthodontic case. Pretreatment diagnosis would save many of these cases and keep the attorneys at bay.
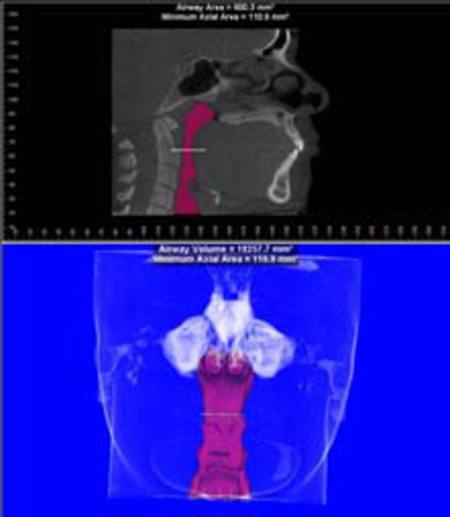
Airway
Picture this...a patient presents on referral from the otolarygologist following episodic jaw pain, cervical pain, fatigue and joint sounds, a classic presentation for temporomandibular disorders. Imaging reveals degenerative joints, pan sinusitis and a collapsed airway. Upon further questioning the patient relates a history of classic sleep apnea symptoms and metabolic syndrome (hypertension, thyroid deficiency and type II diabetes). This combination of potential life threatening disorders that left undiagnosed and treated decreases the patients lifespan and quality of life. Here is where the line blurs between medicine and dentistry. I am responsible to inform this patient of the consequences, initiate referral to appropriate medical specialties and spend quite a bit of unreimbursed time explaining this to the patient. I'm glad to do it and patients are extremely grateful, frankly it is quite satisfying, but is this better left to the physician? And in our capitated medical model how long is the referral going to take?
Let's rattle off a few more: Childhood airway issues...highly under diagnosed, leading to postural issues, malocclusion, sleep apnea, ADDHD, enuresis, poor cognition and obesity
Adult airway issues, undiagnosed atheromas, neoplasms, failing root canals, fibrous dysplasias... the list is as long as the index in the pathology book collecting dust on your shelf.
I applaud my referring physicians and dental colleagues. They get it. They embrace it despite the fact that the medical IPA may lose money referring outside the system. Most of them realize that conventional CT is a gross overexposure and not as diagnostic for oral and maxillofacial issues. MRI is expensive and not as comprehensive in diagnosing DJD and airway issues. Some ENT groups value this so much they are incorporating the technology into their own office. Nancy Haley Appleblatt. M.D, a well regarded Sacramento ENT has this to say "the miniscanner/ CBCT gives me complimentary information in the axial, coronal and sagittal views re: the sinuses, airway and TMJ in a fraction of the time...this patient friendly technology reduces both cost and radiation exposure as compared to conventional CT...In one minute I get a beautiful delineation of sinus pathology with the patient having real time access to the information...being the first ENT practice in the US to have a XORAN scanner in office, has been invaluable to my practice of ENT and Sleep Medicine." Sensationalists will argue about risk/benefit and the overuse of technology as another sign of defensive medicine. This may be true when there is a rumbling among the endodontists that CBCT is necessary for proper visualization of canal space. A brilliant use no doubt, but the success rate of an endodontic procedure is often quoted at 95%. Will the logistical challenges and expense justify wholesale change for a predictable procedure? Collecting images for an implant case, complicated surgical procedures, TMD, sleep and airway volume seem to be more appropriate and can affect outcome in less predictable procedures.
Let's rattle off a few more: Childhood airway issues...highly under diagnosed, leading to postural issues, malocclusion, sleep apnea, ADDHD, enuresis, poor cognition and obesity
Adult airway issues, undiagnosed atheromas, neoplasms, failing root canals, fibrous dysplasias... the list is as long as the index in the pathology book collecting dust on your shelf.
I applaud my referring physicians and dental colleagues. They get it. They embrace it despite the fact that the medical IPA may lose money referring outside the system. Most of them realize that conventional CT is a gross overexposure and not as diagnostic for oral and maxillofacial issues. MRI is expensive and not as comprehensive in diagnosing DJD and airway issues. Some ENT groups value this so much they are incorporating the technology into their own office. Nancy Haley Appleblatt. M.D, a well regarded Sacramento ENT has this to say "the miniscanner/ CBCT gives me complimentary information in the axial, coronal and sagittal views re: the sinuses, airway and TMJ in a fraction of the time...this patient friendly technology reduces both cost and radiation exposure as compared to conventional CT...In one minute I get a beautiful delineation of sinus pathology with the patient having real time access to the information...being the first ENT practice in the US to have a XORAN scanner in office, has been invaluable to my practice of ENT and Sleep Medicine." Sensationalists will argue about risk/benefit and the overuse of technology as another sign of defensive medicine. This may be true when there is a rumbling among the endodontists that CBCT is necessary for proper visualization of canal space. A brilliant use no doubt, but the success rate of an endodontic procedure is often quoted at 95%. Will the logistical challenges and expense justify wholesale change for a predictable procedure? Collecting images for an implant case, complicated surgical procedures, TMD, sleep and airway volume seem to be more appropriate and can affect outcome in less predictable procedures.
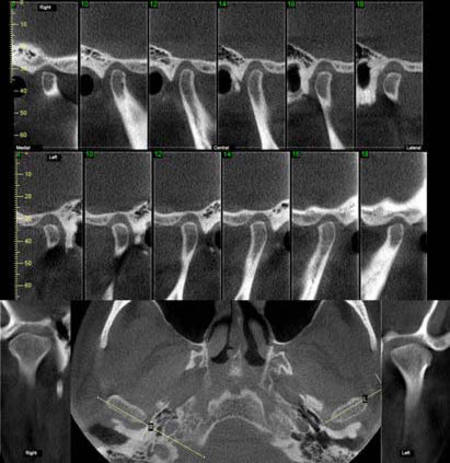
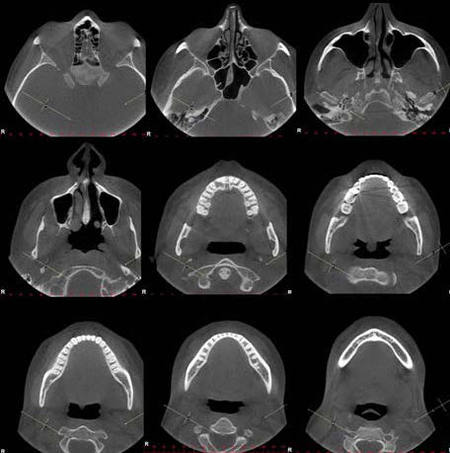
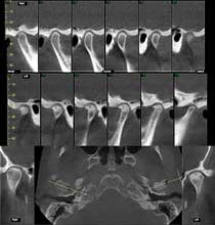
Top & Middle: TMJ Slices Lateral |
Bottom: Axial, Coronals
|
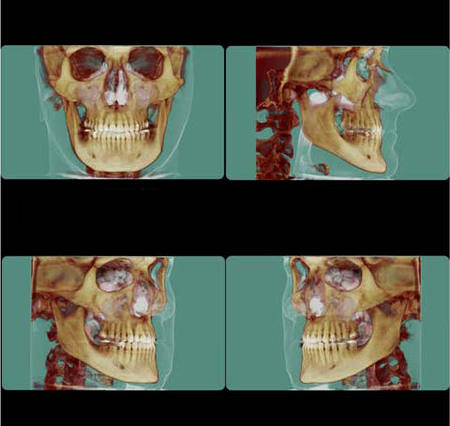
Reconstructed TMJ views, Lateral, Coronal and Axial
|
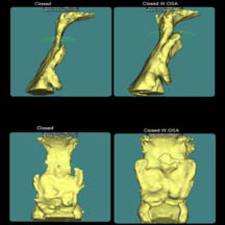
David Hatcher, preeminent maxillofacial radiologist, feels the technology provides an opportunity to utilize a "systems approach, to visualize and evaluate the functional and developmental relationships between proximal craniofacial regions." This functional and growth relationship is an excellent justification for the use of CBCT in orthodontics using anatomic segmentation for morphometric analysis, simulation and biomechanical testing. Indeed there is the ability for 4D and 5D modeling to factor in time and the fusion of genetic, environmental and outcomes prediction (Usui etal., 2003).

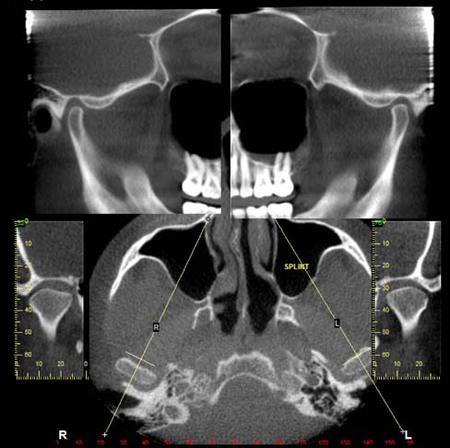
Coronal slices
|

|
The key is education and a patient-centered model. Dentists need to understand that profit driven dentistry and the latest gadget will never make up for great diagnostic technique, compassion and empathy. Physicians need to understand that there are tools that may be out of their comfort zone, yet are more cost effective and better for the patient. Insurance companies need to embrace the efficacy of CBCT. Oral Radiologists and Radiographic Technicians at imaging centers need to step out of their comfort zone and carefully lead this diagnostic revolution. This requires communication with physicians, especially sleep specialists, otolarygologists, and plastic surgeons. In order to set a standard we need more qualified radiologists who understand the stomatognathic system. Continuous education of the orthodontic and oral surgery communities is mandatory. Most importantly the general dentist who has embraced the technology, needs a qualified radiologist and technologist to aid in the interpretation. Logistically this can be a huge issue for those in rural areas, or perhaps they are unaware of the diagnostic groups available. This too may be economy driven as dentists look for profit centers without realizing the complexity of the technology. Share your expertise despite "competition" from the local dentist struggling with the technology. Each day I tell myself "you only compete with yourself." There is liberation in cooperation. Burst the bubble.
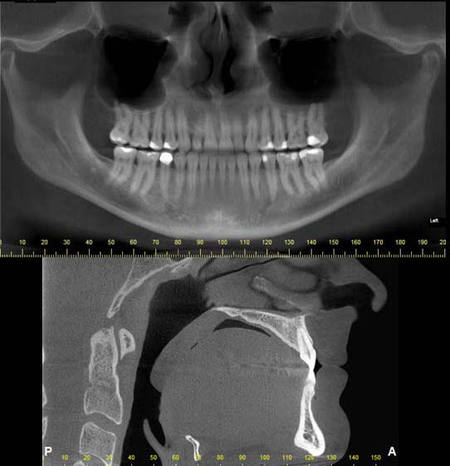
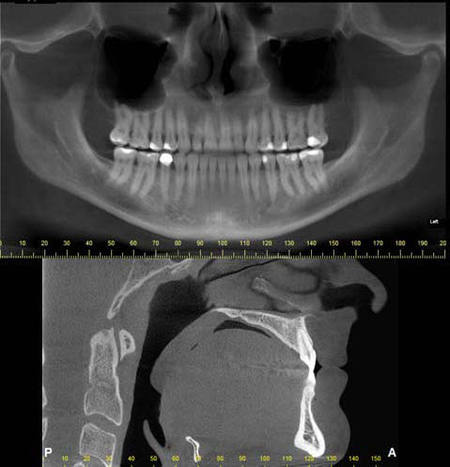
Reconstructed Panoramic and Midline/Airway
|
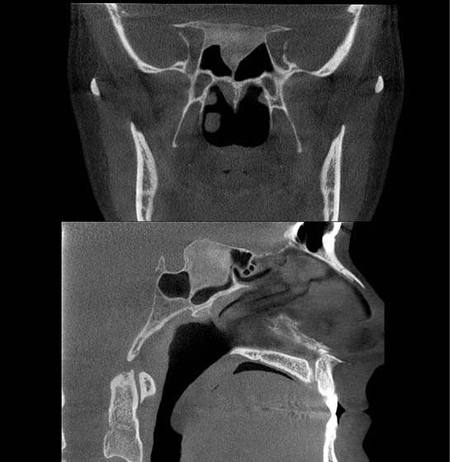
Coronal Airway and Midline/Airway
|
RADIOGRAPHIC REPORT
Observations:
Observations:
|
MISSING TEETH:
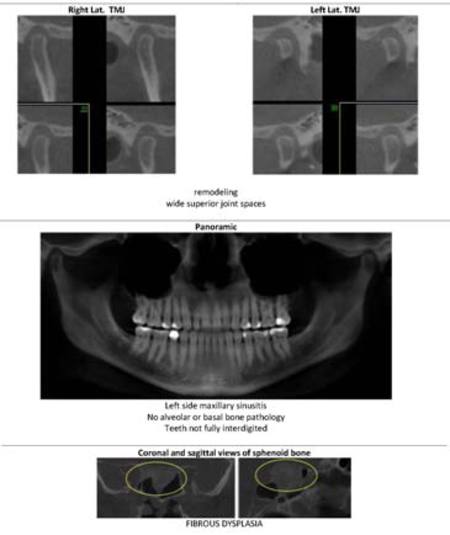
SINUSES: SPHENOID BONE: TMJS: OCCLUSION: AIRWAY: |
#s 1, 16, 17 and 32.
A fluid level, consistent with inflammatory sinus disease, was noted in the left maxillary sinus. The anterior clinoid process and adjacent portion of the sphenoid have been enlarged. Internally there was a granular bone pattern. The superior surface of the condyles showed signs of flattening and sclerosis. An osteophyte was extending from the anterior surface of the condyles. When the mandible was in the closed position the condyles were located inferior to the center of their fossa and the resultant superior joint spaces were wide. When the appliance was in place the condyles were centered within their fossa. There was a class III occlusion with an anterior end to end tooth contact. The posterior teeth were not fully interdigitated. The dimensions of the airway, posterior to the soft palate and tongue base, were within normal limits. |
Impressions:
|
TMJs:
SPHENOID BONE: |
The structure and morphology of the osseous components of the TMJs were evaluated and the findings noted above were consistent with remodeling. The remodeling was at an intermediate stage and may be a response by the articular tissues to the functional demands. The demonstrated closed mouth condyle/fossa spatial relationships were acquired (i.e., condyles not seated within their fossa) and may be the result of a dual bite or diplacement of the condyles.
The sphenoid bone had a bone pattern consistent with fibrous dysplasia. |
Biography
Dr. Timothy Mickiewicz maintains a comprehensive restorative practice in Sacramento, CA. He is a Diplomate of the American Academy of Pain Management and maintains one of the few accredited orofacial pain programs in the country. Dr. Mickiewicz has spent the past twenty years developing a model for the incorporation of complex TMD and Sleep Medicine patients into dental practices. A recognized leader in the field, the practice has unique contracts with major medical groups throughout Northern California. His innovative approach lead to the approval of TMD Splints, Dental Sleep Appliances and CBCT by the medical insurance industry. He has been happily married for 31 years with three grown children, and he has been a fixture in the community at large. Dr. Mickiewicz is a member of the local, state and national dental societies as well as the National Sleep Foundation and the American Academy of Dental Sleep Medicine.
Dr. Timothy Mickiewicz maintains a comprehensive restorative practice in Sacramento, CA. He is a Diplomate of the American Academy of Pain Management and maintains one of the few accredited orofacial pain programs in the country. Dr. Mickiewicz has spent the past twenty years developing a model for the incorporation of complex TMD and Sleep Medicine patients into dental practices. A recognized leader in the field, the practice has unique contracts with major medical groups throughout Northern California. His innovative approach lead to the approval of TMD Splints, Dental Sleep Appliances and CBCT by the medical insurance industry. He has been happily married for 31 years with three grown children, and he has been a fixture in the community at large. Dr. Mickiewicz is a member of the local, state and national dental societies as well as the National Sleep Foundation and the American Academy of Dental Sleep Medicine.
|
|

|

|