
The Next "Revolution"Ivan Dus, MD, PhD, DDS
University of Rome (Sapienza) University of Barcelona Loma Linda University in California Assistant Professor of Orthodontics From the Fall 2003 AADMRT Newsletter  Dr. Ivan Dus Dr. Ivan Dus
What really happened that is new in orthodontics in the last 50 years? After the event of lateral head x-ray film and cephalometrics, there have not been many real diagnostic tools developed that have been valuable in orthodontic diagnosis and treatment planning. Orthodontic manufacturers have spent most of their effort in developing mechanic tools such as better bands and the event of direct brackets have simplified mechanics tremendously. In the last 2 decades material technology has developed better wires. I have been in orthodontics for over 20 years and every time I made, and still make "mistakes", they are never related to inappropriate mechanics but to inappropriate diagnosis. Ask yourself these questions:
For this reason we have many different "vertical" approaches to orthodontics; techniques like the Tweed, Ricketts, Beggs, or some others defined as per the mechanics itself like straight wires, segmented, functional, etc. We have the tendency to say that the mechanics have failed when in fact we failed to accomplish the treatment. Is it really true? When we define our treatment objectives for our orthodontic treatments, are these objectives really achievable? Mostly in orthodontics we move teeth through anatomical structures, some of them are inviolable sites like: cortical bone, nerve canals, etc. Of course function and behaviors can limit our treatment objectives as well, but we leave this out at the moment to take the structures more into consideration in this specific "talk". |





|
People speaking the same language don't have problems calling an apple an apple once they see it. Even when they speak different languages they can still define the proper object even if they use different words. This is because the object is "visible" in its real appearance and therefore there is no need for interpretation. If orthodontists would have had the opportunity to really be able to see the real anatomical structure to where they have to move the teeth through, would you think that they would have spent all this time arguing on cephalometric techniques or being so religious to mechanics? I don't think so!
Dr. Carl Gugino and myself have spent the last 20 years trying to apply technologies in various areas of orthodontics like understanding muscle function behaviors and breathing dysfunctions. We have developed specific methods and applications using technologies already available in other fields inside and also outside medicine. We have developed our own applications and protocols to assess and treat these dysfunctions. A big obstacle to overcome was how to get specific information about anatomical structures in 3 dimensions. Of course CAT scans have been available in the market in the past 20 years or more, but in order to investigate anatomical structures related to orthodontic diagnosis and treatment planning, we need specific projection that are more related to coronal and sagittal planes. To obtain this with a CAT scan a very dense acquisition would be necessary and this means a huge amount of radiation exposure to our patients. Since the majority of our patients are children, this is neither justified nor practical when cost is added to this. For this reason over the years I have resisted to use CAT scans or to buy my own CAT scan.
So if you had the nerve to read to this point then I will share with you how I came across what I call "the next revolution" in orthodontics.
It was 1998 when I discovered the NEWTOM. The Newtom was "born" as a challenge taken by an Italian company working in the field of x-ray technology. They needed to develop a volumetric x-ray machine to be devoted to dental implantology that had to have 2 major requirements:
Dr. Carl Gugino and myself have spent the last 20 years trying to apply technologies in various areas of orthodontics like understanding muscle function behaviors and breathing dysfunctions. We have developed specific methods and applications using technologies already available in other fields inside and also outside medicine. We have developed our own applications and protocols to assess and treat these dysfunctions. A big obstacle to overcome was how to get specific information about anatomical structures in 3 dimensions. Of course CAT scans have been available in the market in the past 20 years or more, but in order to investigate anatomical structures related to orthodontic diagnosis and treatment planning, we need specific projection that are more related to coronal and sagittal planes. To obtain this with a CAT scan a very dense acquisition would be necessary and this means a huge amount of radiation exposure to our patients. Since the majority of our patients are children, this is neither justified nor practical when cost is added to this. For this reason over the years I have resisted to use CAT scans or to buy my own CAT scan.
So if you had the nerve to read to this point then I will share with you how I came across what I call "the next revolution" in orthodontics.
It was 1998 when I discovered the NEWTOM. The Newtom was "born" as a challenge taken by an Italian company working in the field of x-ray technology. They needed to develop a volumetric x-ray machine to be devoted to dental implantology that had to have 2 major requirements:
- Low radiation exposure
- Low cost of purchase and maintenance
- Immediately when I saw the images, the simplicity of use of the Newtom, and the very low radiation exposure, my brain went on fire thinking about the tremendous opportunity that this machine would have given to me to improve diagnosis and treatment planning in orthodontics. It took me a few minutes to sign the contract and since there was a 90 day delivery time, it was the longest 90 days of my life.
- CONDYLAR TRAUMA (FRACTURE) AND STRUCTURAL DEVELOPMENT DURING GROWTH
- MONO-LATERAL IDIOPATHIC HYPOPLASIC / RESORPTION RELATED TO SYMMETRICAL AND ASYMMETRICAL DEVELOPMENT OF THE BI-MAXILLARY COMPLEX DURING GROWTH.
- BILATERAL IDIOPATHIC HYPOPLASIC / RESORPTION RELATED TO VERTICAL AND HORIZONTAL DEVELOPMENT OF THE FACE
- CONDYLAR / DISK DISPLACEMENT
- ANTERIOR
- POSTERIOR
- LATERAL
- MEDIAL
- LIMITS ON THE SAGITTAL PLANE
- INCISOR
- ADVANCEMENT
- TORQUE
- RETRACTION
- MOLARS & PREMOLARS
- MESIALIZATION
- DISTALIZATION
- LIMITS IN THE VERTICAL PLANE
- INTRUSION
- EXTRUSION
- LIMITS IN THE TRANSVERSE PLANE
- PRE-MAXILLARY COMPLEX
- MAXILLARY COMPLEX
- MANDIBULAR SYMPHISYS
- LOWER POSTERIOR ALVEOLAR BONE
- LIMITS DUE TO AIRWAY OBSTRUCTION (NASAL CAVITY AND EPI-PHARYNX)
- LIMITS DUE TO TONGUE POSTURE
- LIMITS DUE TO THE DISCREPANCY BETWEEN TONGUE VOLUME AND INTRAORAL VOLUME
I have to admit that the impact on volumetric radiology was not natural at all. We have always been exposed to few single flat images, and now having a virtual skull that you can "cut" everywhere, it naturally triggers the curiosity to generate hundreds of different sections of the anatomy. In the beginning I was spending hours on every case, but this has allowed me to later develop specific protocols of sections to evaluate the different areas of interest in orthodontics. The Newtom acquires a volume of 13 cm high, 15 cm wide and 15 cm deep. This at the beginning seemed to be a limitation since we have in our mind the vision of the cephalometric area. This obstacle was overcome very easily just by thinking beyond cephalometrics. Having the opportunity to work with a volume that allows seeing the real anatomy in details and to keep looking for cephalometric measurements, would be like having an airplane that instead of taking off, would just limit itself to taxing on the runway.
For children and adults with small to medium size heads, I was able to get in a single scan all I needed for my diagnostic evaluation. This means from the mandible to the TMJ including most of the airway that are of interest in orthodontics. For larger head size I take 2 scans; one for the bi-maxillary complex and one upper for TMJ and airway. Since I have eliminated all the other conventional records; head film, panoramic, TMJ tomography, periapicals, etc when adding up the radiation exposure of all these conventional x-rays, even 2 Newtom scans is delivering far less radiation than all these together.
ANATOMICAL AND FUNCTIONAL LIMITATIONS IN ORTHODONTICS
I have outlined the following classifications that will allow a better understanding of the different problems that are common in every day orthodontic practice.This article will take into consideration only a few examples from this list.
LIMITS DUE TO TMJ CONDITION
LIMITS DUE TO TMJ CONDITION
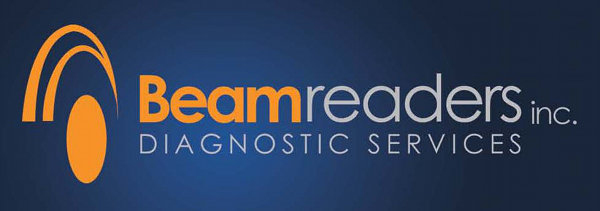
A dolico-facial growth pattern (high vertical and retruded mandible) is very often the expression of a TMJ problem during growth. How many times during an orthodontic treatment when the facial axis suddenly opens sometimes with no reason do we blame the extrusion of posterior teeth? Condyle growth dysfunction is more common than what we may think. Conventional radiology, tomos included, has no way of showing this problem since in the early stages it is detectable only in the coronal plane by evaluating the condyle morphology and its relation with the fossa in maximum intercuspidation.
One example:
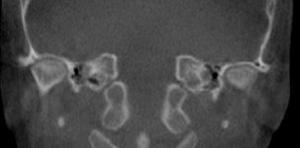
Figure 1

Figure 2
- This 9 year old boy (Figure 1, 2) shows a dolico pattern and a retruded mandible. The coronal images of the TMJ part of one Newtom single acquisition), shows morphological alteration of the condylar profile and very limited peri-condylar space, both at the lateral and medial pole. This situation indicates that both disks are displaced causing blood supply limitation to the condyle head and therefore interfering with growth and development.
LIMITS DUE TO STRUCTURAL CONDITION
Height of alveolar bone
Moving teeth sometimes can become a challenge; very often we have the tendency to blame the patient for their lack of cooperation. Sometimes this can be the case, but often the problem is hidden outside the possibility to "see" with conventional records.To try to correct this overbite (Figure 3, 4) by intruding the upper incisors it is a lost war right from the beginning. If the situation is forced using intrusion mechanics, there is a risk for apical trauma, tooth necrosis or root resorption.
Figure 3
|

Figure 4
|
Lateral (Figure 5), panoramic or periapical x-rays, don't give any attainable indication about this structural limitation. We can only become aware of this when we fail the objective of our treatment or we get root resorption. Despite this, without the Newtom Image, the real cause of the failure will never be determined.

Figure 5
- Distalization and mesialization of molars and premolars
Asymmetric dental relation (dental class) between right and left side is a frequent condition of orthodontic patients. The causes are varied and the most critical follow: a) different relation and development of the maxillary sinuses between right and left side; b) different timing in the eruption of permanent teeth in relation to their mesialization, thus creating a posterior space by teeth already erupted; c) problems related to asymmetrical growth of the TMJ or displacement of the articular disk on one side with the on sequence of posterior dislocation of the condyle on the same side.
Using volumetric radiology, it is possible to immediately evaluate the feasibility of distal or mesial movement of the teeth. Understanding the concept of "spatial location" will facilitate planning of orthodontic treatment with fewer errors. It also provides an immediate forecast of stability over time yielding a more reliable retention period.
The distance 6-PTV is well known to orthodontists, especially those possessing a Bioprogressive background. This is an empirical measurement based on a landmark not always easy to locate in a traditional lateral X-ray film. The error margin relates to the different spatial positions between the merging point of the Foramen Rotondo (Pt point) and the position of the molars in the coronal plane.This distance changes with age and facial morphology, it is less precise during growth (increase of A distance between the effective position and projected point in the lateral X-ray).

Figure 6
|

Figure 7
|
Another index of 6-PTV error is the varying size of the pterigo-maxillary space related to facial morphology. Understanding the correct inclination of the teeth and the relation of the roots with the floor of the maxillary sinuses and the anterior wall of the sinuses (especially for the premolars), will allow evaluation of the possibility to move the teeth; particularly the movement ratio between the root and the crown. Sometimes correcting a class II can be relatively easy. If we take the time to investigate, utilizing volumetric radiology data, we find the crowns of the teeth mesially inclined and probably mesio rotated. On the contrary, the difficulty correcting a class II is the distal inclination of the crown.
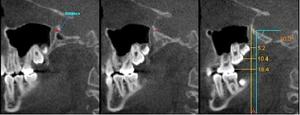
Figure 8
The pterigo-maxillary suture has a different relationship between a growing person (Figure 10) and an adult person (Figure 9). In a child the Pterigoid lamina is medially located to the maxillary tuberosity and it moves (rotates) externally during growth. Notice there is no available space posteriorly, the most posterior tooth will always be against the posterior wall of the maxillary tuberosity.

Figure 9
|
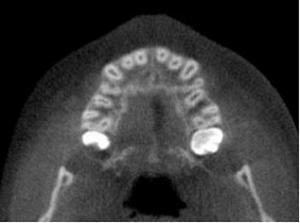
Figure 10
|
- How does a dental class II develop? Thanks to the investigation conducted with volumetric radiology we are able to understand more about these mechanisms. The speed in which teeth erupt is in direct relation to the space available. A premature mesialization of the posterior denture will allow for more space available on the tuberosity level, stimulating the eruption of the posterior teeth. In this way, a temporal discrepancy is established between the eruption and mesialization of the upper and lower arch, resulting in the development of a class II. The problem is of course more complex, but it cannot be fully intimated in this limited space.
LIMITS DUE TO DYSFUNCTIONAL CONDITION
Discrepancy Between Lingual Volume and Intraoral Volume
Lingual volume is not always adequate to maintain the equilibrium between intra and extra-oral forces. This is particularly true during cranio facial development. If intra-oral volume increases as the result of posterior mandibular rotation, this will be compensated by increasing alveolar height. The tongue volume does not compensate for this as its volume is genetically determined and function does not affect it. The discrepancy between tongue and intraoral volume is a different condition than tongue postural dysfunction based on oral breathing, habits or a tight lingual frenulum. These patients usually have both arches constricted and are more difficult to treat. Particularly, after maxillary expansion, these patients need to be retrained over time to avoid relapse.
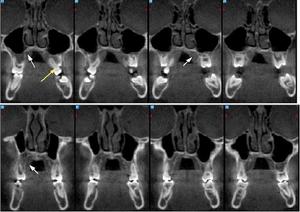
Figure 11
These images (Figure 11) are sections from an acquired volume and very clearly indicate many aspects of this problem. First of all, notice the height of the roof of the palate and the thickness of the palatal mucosa (white arrow) as a result of absence of the pressure exerted by the tongue during swallowing. It is easy to see the empty space the tongue is unable to fill. In the posterior part of the maxilla, there is a negative inclination of the molars (yellow arrow). This condition limits orthodontic expansion treatment. To maintain the expansion, retention over a period of time is essential.
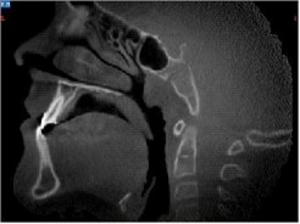
Figure 12
- This image (Figure 12) represents a sagittal section of the same patient. Observing the relationship of the tongue with the maxilla and the mandible, it is very conclusive the understanding of the structural problems related to the swallowing and tongue posture dysfunction.
Adeno-Tonsil Hypertrophy
In the past, several authors attempted to measure the respiratory space delimited by the anterior part of the adenoid tissue and the posterior part of the soft palate. This method of evaluating the epipharingeal space, aside from being inadequate, has been a source of dispute between ENT and orthodontists. In reality, adenoid obstruction happens when the adenoid tissue develops anteriorly toward the posterior nasal aperture, and penetrates to touch the posterior tails of the lower turbinates (green arrow.) This condition is responsible for the mechanical obstruction of the airway. When the adenoids are so large, they interfere with the Eustachian tubes and alter the pressure regulation and ventilation of the mid ear. This is a frequent cause of recurrent otitis.
Volumetric radiology exam.
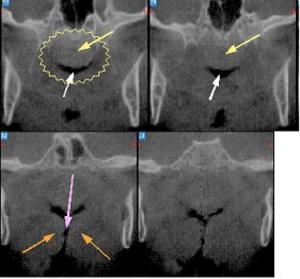
Figure 13
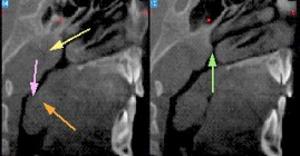
Figure 14
- These are some coronal and sagittal sections selected from a series of transaxials. These very clear images are part of the standard acquisition volume available for every patient. The white arrow points to the posterior breathing aperture. The yellow arrow points to the adenoid tissue (inside the yellow circle). The orange arrow points to the hypertrophic tonsils. The purple arrow points to the restricted pharingeal-laringeal passage resulting from tonsilar hypertrophy.
We have only considered a very few examples of the problems that we need to face in an everyday orthodontic practice. There are many many more, not to mention the dilemma with impacted teeth. Is it possible to recuperate orthodontically an impacted cuspid? This can be a very challenging evaluation to make. The Newtom with its volumetric capabilities will allow evaluating that tooth in all the planes not only through sections but also using real 3D images that you can rotate, "peel off the bone" and determine the relations with other teeth or adjacent structures.
These pictures (Figures 15-19) represent just an example of an impacted cuspid. Because the apex of the root is away from the cortical bone between the nose and the maxillary wall, and the fact that the alveolar bone height is appropriate, it is possible to recuperate this tooth orthodontically. The surgical path and the orthodontic fixation of the tooth are also very easy to determine just by evaluating these images.

Figure 15
|

Figure 16
|

Figure 17
|

Figure 18
|

Figure 19
|
There is no doubt that the Newtom brought a new dimension into orthodontics. What is needed from our side as clinicians is an open mind to accept the learning curve that there is to it. Once you get there it will be impossible to "live" without the diagnostic and treatment capability that the Newtom with its volumetric capabilities, ease of use, and very low radiation exposure to the patients, can offer.