
Utilization of CBCT in an Orthodontic PracticeDavid L. Way, D.D.S., M.S.
Private Practice of Orthodontics Fort Collins, Colorado From the Summer 2006 AADMRT Newsletter  Dr. David L. Way Dr. David L. Way
What I would like most as an orthodontic practitioner conducting an initial examination would be a crystal ball providing me with a glimpse of the future for each individual. If the patient is not yet mature I would want to know their final growth outcome including cranio-facial skeletal relationships, and for all individuals I would want to know if there was any pathology present, temporal-mandibular joint health, periodontal health status and adequacy of airways. I would also want to know if they had dental stability and if the wear on their dentition was within the range of normal or accelerated due to a malocclusion and/or para-function.
Short of having a crystal ball I want access to all of the diagnostic information possible for an initial examination. A great deal of information can now be provided with the utilization of Cone Beam CT (CBCT). I may not know the future but I can more reasonably predict possible treatment outcomes by having a greater wealth of diagnostic information as well as access "diagnostic truth". This wealth of information is provided at a very reasonable exposure to the patient and is very easily obtained. One CBCT scan gives me exponentially more data (and more accurate data) than the combination of a panogram, lateral cephalogram, PA cephalogram and spiral or linear tomography. With the addition of CBCT into our practice, patient flow has changed very little. The most significant change is not having to schedule a second appointment for the acquisition of temporalmandibular tomograms which were much more time consuming and the quality of the films were much more operator dependent. The information provided on TM joints with CBCT is more comprehensive and much more accurate (diagnostic truth). Never before have we been able to evaluate airways as thoroughly as we now do on a daily basis. The other obvious advantages include but are not limited to determining the position of roots within the alveolar trough in all planes of space, screening for head and neck pathology, nerve location, adequacy of bone for future implants, diagnosing ectopically erupting teeth and evaluating the proximity and quantity of bone in our cleft palate patients. Patient Flow and integration of CBCT into the orthodontic initial examination process: |





|
- Patient fills out health hx on-line or fills out paper form
- Forms include TMD and airway screenings
- Meet and greet by Treatment Coordinator (TC) describing exam sequence including CBCT
- CBCT taken in Centric Relation (CR)-other staff import dicom files into Dolphin 3D to build cephalograms
- Photos taken by TC in CR
- TC meets with Dr. in office to review patient health hx/ screenings while Dr. Reviews CBCT and digitizes cephalograms in Dolphin 3D
- Dr. meets patient, interviews patient, TMJ clinical exam, airway screening and facial measurements taken along with occlusion examination.
- Dr. reviews findings and treatment recommendation with patient
- Dr. leaves room and TC concludes examination process and schedules necessary appointments
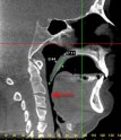
Prior to seeing the patient, the tri-planner view of the CBCT is screened for any observable pathology. This is something we were only able to do in a limited manner with two-dimensional radiographs looking through a great depth of anatomy with inherent distortion due to the manner in which the image was obtained.
|
|
|
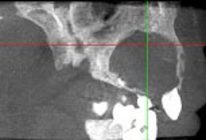
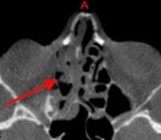
The second task is to review the tri-planner view examining the airways. This includes the retro-glossal airway, retropalatal airway, nasal passageways and all sinuses. Adequacy of airways can affect skeletal growth patterns in growing individuals and can also affect dental stability in growing as well as non growing individuals. The airways are also a reflection of skeletal relationships and can give us a clue of those individuals that may have or be at risk for sleep disorders including obstructive sleep apnea. In addition, we will sometimes find sinus polyps, maxillary sinus infections and even ethmoid sinus disease. Upon finding pathology, the appropriate referrals are made accompanied by a video copy of the CBCT on a CD.
|
|
|
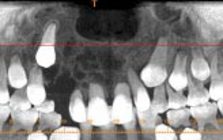
The third task is to screen for periodontal health. This includes the position of roots within the alveolar trough, relative horizontal bone levels and root proximity. Until the voxel size reaches .1mm, peri-apical films will still be needed by the periodontist for clarity, but only the CBCT can allow us to traverse each arch showing us root positions in all three planes of space. This is the point where I will also examine the views of ectopically erupting teeth as well as impacted teeth.

|

|
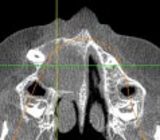
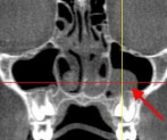
Asymmetries are the next facet of diagnostic information I will observe while I am still in the tri-planner view of the CBCT. Recognizing asymmetries and developing asymmetries is an extremely important part of the orthodontic diagnostic process as this has profound affects upon how we plan for the individual?s treatment.

|

|
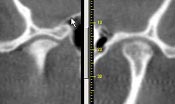
Following the tri-planner investigations, I will then build the TMJ studies examining form, volume and position of the condyles within the fossa as well as the anatomy of the fossa itself. Because our patients have either completed their health history questionnaires on-line or in our office prior to my review of all of the above I am able to add this information to the diagnostic information provided by the CBCT and the information obtained by my treatment coordinator all before I have even met my patient. To have this information at my initial exam only enhances the diagnosis, treatment planning, and educational process.
|

|
Prior to my viewing the CBCT volume in the proprietary software another staff member takes a "step backwards in time" and builds 2D lateral and posterior-anterior cephalograms in Dolphin 3D (orthodontic imaging software) to allow me to digitize the cephalograms and provide me with further diagnostic and treatment planning information. This process is at this time a necessity for the orthodontist but 3D digitizing will soon be here and in fact is being developed and tested at this time. The quality of the cephalograms built from the CBCT is without a doubt a huge improvement over the conventional 2D radiographs. The CBCT and extra-oral photographs are taken with an operator assisted first tooth contact centric relation wax bite registration. We can make more appropriate treatment decisions as opposed to images taken in habitual jaw positions that may not reflect the true relationship of the mandible to the maxilla and thus may inaccurately reflect condylar position and the relative dental relationships.
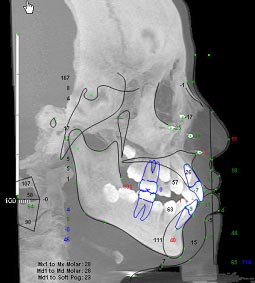
The superior diagnostic information provided by CBCT over conventional radiographic technology dictates that we make the transition form 2D diagnosis and treatment planning to 3D sooner rather than later. Most all of us have inherent asymmetries and skeletal discrepancies but the greater the magnitude of these discrepancies the more important 3D imaging, digitization and treatment planning becomes. For example, treatment planning of orthognathic surgical cases in 3D will provide us a more complete picture of treatment options and projected treatment outcomes, which in the end is a huge benefit for the patient.
Effective communication is an important aspect of this technology that cannot be underestimated. Communication is an essential part of what we do each day. Improving communication with the patient, the referring doctor and to those to whom we refer our patients should always be our goal. You can be confident in the patient?s ability to understand what is being shown to them when looking at the tri-planner view as well as 3D modeling. This is especially true when providing examples of normal anatomy as a comparison.
Effective communication is an important aspect of this technology that cannot be underestimated. Communication is an essential part of what we do each day. Improving communication with the patient, the referring doctor and to those to whom we refer our patients should always be our goal. You can be confident in the patient?s ability to understand what is being shown to them when looking at the tri-planner view as well as 3D modeling. This is especially true when providing examples of normal anatomy as a comparison.
Providing ENT?s with a three-minute video copy of scanning through the tri-planner view of the CBCT is one example of improved communication. This is accompanied by a short letter and voice narration on the CD, which very effectively communicates the reason for the referral and what information I am looking for in return. This not only builds strong professional relationships but also provides better and more comprehensive care for our patients.
The future is bright for this technology. I feel we are only now scratching the surface of its possibilities. Decreasing voxel size, being able to visualize other data that has been captured in CBCT such as nerves and vessels, being able to quickly and accurately determine volumes of airways and other anatomy and improving the merging of 3D photos with the radiographs are all examples of projects being worked on at this time. I am confident we will see the benefits of these projects sooner rather than later.
We cannot be afraid of new technology that provides us with infinitely more diagnostic data. We have to embrace it and increase the scope of our diagnostic abilities and incorporate this data into our everyday treatment planning. The bottom line is that we have an opportunity to improve our patient care.
The future is bright for this technology. I feel we are only now scratching the surface of its possibilities. Decreasing voxel size, being able to visualize other data that has been captured in CBCT such as nerves and vessels, being able to quickly and accurately determine volumes of airways and other anatomy and improving the merging of 3D photos with the radiographs are all examples of projects being worked on at this time. I am confident we will see the benefits of these projects sooner rather than later.
We cannot be afraid of new technology that provides us with infinitely more diagnostic data. We have to embrace it and increase the scope of our diagnostic abilities and incorporate this data into our everyday treatment planning. The bottom line is that we have an opportunity to improve our patient care.