
Imaging in endodonticsSam Alborz, DDS
Endodontist Private Practice Knoxville, TN From the Winter 2008 AADMRT Newsletter  Dr. Sam Alborz Dr. Sam Alborz
Radiography has always played a big part in endodontic treatment. Traditionally in endodontics, radiographs are used for diagnostic, intra-operative, post-operative, and recall appointments. Although imaging in dentistry has greatly advanced recently, the most common images used in endodontics are the periapical and bitewing radiographs. The area where technological advances have been utilized the most by endodontic practices is digital imaging. Many endodontic practices are moving from the film based intraoral radiographs to digital radiographs. Digital radiography is fast becoming the preferred technique over traditional film based images due to the speed of obtaining the image.
Using CCD and CMOS sensors, the practitioner is able to view the images immediately after exposure which is vital to intraoperative radiographs during root canal treatment. This is crucial when dental materials such as a rubber dam and files are present in the patient's mouth while imaging. Preoperatively, using the periapical image, the endodontist is able to view the tooth being diagnosed with fine detail including the crown, roots, periodontal ligament space and surrounding bone (Fig. 1). The diagnostic applications of the endodontic image include: determining the proximity of restorations to the pulp chamber, presence of periapical or periradicular pathology, presence of pulp stones, presence of separated instruments within canals, quality of previous endodontic treatment, and possible detection of a fractured root. 
Figure 1: Tooth #30 is seen here with an under-prepared and under-filled root canal treatment. Tooth #31 has a large carious lesion and fractured restoration. Either one of these teeth could be the source of discomfort to the patient.
|





|
Intra-operatively, radiographs are used to determine the length of the canals and the gutta percha cone fit to the apices. These films are taken with the file or cone placed in the canal(s) (Fig. 2 a-b). However, with the advent of the Electronic Apex Locator, the need to take a length film has been reduced significantly. Most of the time one can rely on accurate measurements of the true biological apex of the canal using the apex locator. Nevertheless, there are times such as in the case of a metal crown, bleeding, or a long standing periapical abscess, that the apex locator fails to provide an accurate measurement thereby requiring a radiograph to determine length.

Figure 2(a): Shows length determination using files in the canals.
|

Figure 2(b): Shows the cone fit radiographs to determine the fill relative to the apices.
|
Post-operatively, radiographs are used to check the quality of the obturation (fill) and are used as a baseline reference for the recall appointment. For example if a periapical lesion was present preoperatively (Fig. 3), the size and location would be recorded radiographically and could be checked during recall visits to ensure extent of healing and resolution of the lesion. The radiographs may also show if there is gutta-purcha or sealer extruded beyond the apex and the patient can be informed of possible post-operative sensitivity.
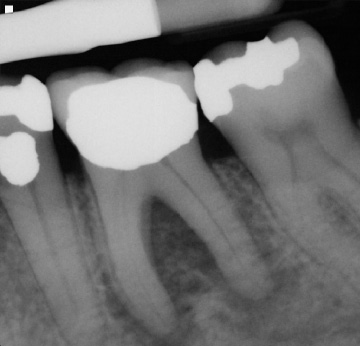
Figure 3: A pre-operative radiograph of a tooth with a radiolucent lesion of endodontic origin.
|

Figure 4: Shows completion of the root canal treatment.
|
Recall visits are extremely important in endodontics as it is often through the radiographic healing that we measure success of the treatment. Although the patient may not present with symptoms at the time of recall, the radiographs may reveal a periapical lesion remaining. In those cases the endodontist may have to choose retreatment or surgery (Fig. 5).

Figure 5: One year recall of the same case in Fig 3 & 4, showing complete healing and resolution of radiolucency.
The SLOB Rule
The SLOB rule is one of the most widely used radiographic concept in endodontics. On periapical radiographs, roots are often superimposed upon one another and require separation for proper identification. The SLOB rule is an acronym for Same Lingual Opposite Buccal. The premise is that one radiograph is taken straight on at a 90 degree angle to the tooth and a second radiograph is taken with the tubehead shifted either mesially or distally. The rule simply states that the object imaged will move in the same direction as the tubehead is moved if it is located on the lingual (Same Lingual). Conversely, the object being imaged will move opposite the tubehead movement if it is located on the buccal (Opposite Buccal). An example of this would be a palatal root, which is on the lingual side of a maxillary molar, will move mesially on the image if the tubehead moves mesially (Same Lingual).
During root canal treatment the endodontist may need to separate the canals to visualize lengths and anatomy. Another important application of this rule would be in the case of a separated instrument. It is quintessential to know which canal the instrument is in for both clinical and documentation purposes. Sometimes just changing the angulation of the beam can aid in identifying factors that are not visible on the straight (perpendicular) shot. Those findings can include root fractures, additional roots or canals etc. The key to this technique is to remember which direction the tubehead was angulated on the second radiograph since the image receptor may not be placed in the exact location of the first image (Fig. 6 a-b & 7 a-b). Labeling the radiographs can help alleviate any doubt and will help in archiving the images. Images can be simply labeled as "straight" for the first and "mesial" or "distal" for the off-angled image. If using film, it is easy to label the images by just using a 2 hole mount and a wax crayon or pencil. Most digital images can be labeled by adding a text box or using the tools available in the software to add notes. Training the staff to use the same system also aids in consistency of the technique and proper archiving of the images.
The SLOB rule is one of the most widely used radiographic concept in endodontics. On periapical radiographs, roots are often superimposed upon one another and require separation for proper identification. The SLOB rule is an acronym for Same Lingual Opposite Buccal. The premise is that one radiograph is taken straight on at a 90 degree angle to the tooth and a second radiograph is taken with the tubehead shifted either mesially or distally. The rule simply states that the object imaged will move in the same direction as the tubehead is moved if it is located on the lingual (Same Lingual). Conversely, the object being imaged will move opposite the tubehead movement if it is located on the buccal (Opposite Buccal). An example of this would be a palatal root, which is on the lingual side of a maxillary molar, will move mesially on the image if the tubehead moves mesially (Same Lingual).
During root canal treatment the endodontist may need to separate the canals to visualize lengths and anatomy. Another important application of this rule would be in the case of a separated instrument. It is quintessential to know which canal the instrument is in for both clinical and documentation purposes. Sometimes just changing the angulation of the beam can aid in identifying factors that are not visible on the straight (perpendicular) shot. Those findings can include root fractures, additional roots or canals etc. The key to this technique is to remember which direction the tubehead was angulated on the second radiograph since the image receptor may not be placed in the exact location of the first image (Fig. 6 a-b & 7 a-b). Labeling the radiographs can help alleviate any doubt and will help in archiving the images. Images can be simply labeled as "straight" for the first and "mesial" or "distal" for the off-angled image. If using film, it is easy to label the images by just using a 2 hole mount and a wax crayon or pencil. Most digital images can be labeled by adding a text box or using the tools available in the software to add notes. Training the staff to use the same system also aids in consistency of the technique and proper archiving of the images.

Figure 6(a): Separated instrument in one of the mesial canals.
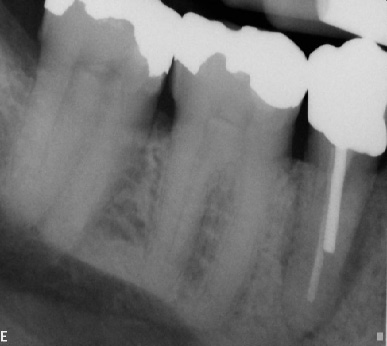
Figure 7(a): Tooth #29 with periradicular radiolucency and previous root canal. At first glance it appears as though there may be a recurrent infection.
|
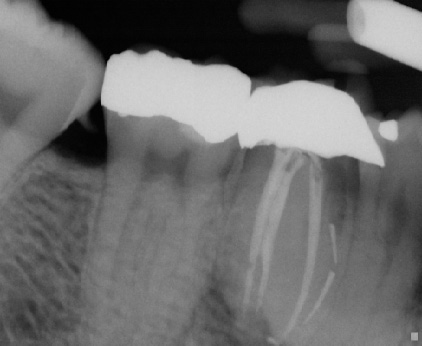
Figure 6(b): Distal angle radiograph reveals instrument is in the Mesio-Buccal canal as the instrument has shifted more to the mesial (Opposite Buccal); note the distance between the filled mesial canal and the separated instrument increased.

Figure 7(b): An angled radiograph reveals that the root is fractured.
|
Clinical Case
Patient presented for root canal treatment on tooth #14. The canals were extremely calcified and after three visits we were able to complete the case (Fig. 9 a-b). Convinced that we had provided the best possible treatment for the patient and were able to find all of the canals the patient was discharged only to return three months later with recurrent pain. Upon careful examination she expressed tenderness upon biting and palpation of the mesiobuccal root. A distal angle radiograph revealed a wide mesiobuccal root indicating a possible additional canal in that root (Fig. 10). The case was accessed and the canal was found and treated (Fig. 11)
Patient presented for root canal treatment on tooth #14. The canals were extremely calcified and after three visits we were able to complete the case (Fig. 9 a-b). Convinced that we had provided the best possible treatment for the patient and were able to find all of the canals the patient was discharged only to return three months later with recurrent pain. Upon careful examination she expressed tenderness upon biting and palpation of the mesiobuccal root. A distal angle radiograph revealed a wide mesiobuccal root indicating a possible additional canal in that root (Fig. 10). The case was accessed and the canal was found and treated (Fig. 11)

Figure 9(a): Pre-op radiograph, note the extent of calcification of the canals.
|

Figure 9(b): Case completed.
|

Figure 10: Showing wide mesiobuccal root (red arrow).
|

Figure 11: Clinical photo showing the additional canal, cleaned, shaped, and obturated (filled).
|

Figure 12: Clinical photo showing the additional canal, cleaned, shaped, and obturated (filled).
|
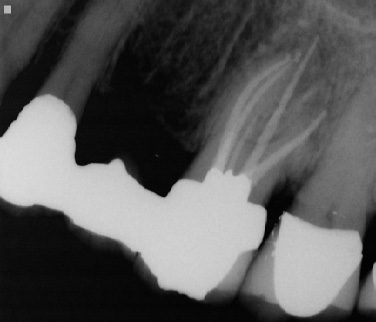
Figure 13: Showing the final radiograph.
Periapical radiographs still remain the imaging of choice for the endodontist. The convenience of digital radiography for intra-operative periapical radiographs make it an ideal technique to achieve the diagnostic goals stated previously. Although endodontics has used these types of images in the past and present, the future may lend to new techniques. With the technological advancements in Oral Radiology many new imaging techniques are emerging that may supplement the basic techniques currently being used. Imaging such as Cone Beam Computed Tomography (CBCT), which scans patients at high resolution, may aid in pre and post operative imaging. Diagnosing cracked teeth, preparing for apical surgery or searching for missed canals may also be possible using this new treatment modality. For intraoperative procedures however, the digital periapical image remains a great asset.