
Ectodermal Dysplasia: A condition with multiple missing teethSanjay M. Mallya, BDS, MDS, PhD
Diplomate, American Board of Oral & Maxillofacial Radiology UCLA School of Dentistry Los Angeles, CA From the Fall 2011 AADMRT Newsletter  Dr. Sanjay M. Mallya Dr. Sanjay M. Mallya
Failure of tooth formation is a common dental developmental abnormality. In the permanent dentition, the reported incidence of congenitally missing teeth (excluding third molars) is approximately 3% to 10%. The terms hypodontia, oligodontia and anodontia are used to denote the degree of tooth agenesis. Hypodontia refers to developmental absence of one or more teeth in the deciduous or permanent dentition. The most common missing permanent teeth, in order of frequency, are third molars, second premolars, maxillary lateral incisors and mandibular central incisors. When six or more permanent teeth are missing, the term oligodontia is used. Anodontia, congenital absence of both the primary and permanent dentition, is relative rare.
Teeth are derived from the ectoderm - one of the three primordial cell layers in the embryo. Cells in the surface ectoderm differentiate into the epidermis, nails, sweat glands and teeth. Genetic mutations that interfere with this process result in ectodermal dysplasia (ED). These mutations may be inherited as autosomal recessive, autosomal dominant or Xlinked patterns. Several genetic mutations that result in ED have been identified. These include Ectodysplasin (EDA) gene, EDA receptor (EDAR) gene and the NF-β Essential Modulator (NEMO) gene. There are more than 150 clinically distinct hereditary syndromes in which ectodermal dysplasia is present. These syndromes vary in the combination and severity of the manifestations of abnormal ectodermal morphogenesis. The most common form of ED is X-linked hypohidrotic ED. In this disorder, patients have reduced number of eccrine sweat glands. As a result these patients are unable to regulate body temperature and exhibit heat intolerance. Other manifestations include missing teeth, aberrant tooth morphology, thin sparse hair, abnormal nails, frontal bossing, low nasal bridge, maxillary hypoplasia, cleft palate, visual and hearing abnormalities and a thin, atrophic skin. Depending on the type of ED, there is considerable heterogeneity in the severity of the manifestations and patients may not exhibit all of the manifestations. |






|
Congenitally missing and malformed teeth are common manifestations of ED. The lack of teeth compromises not only esthetic appearance but also masticatory function and speech development. To address these functional and cosmetic issues and its consequent psychological implications, patients typically seek treatment early in life. Dental management of ED patients can be challenging and is best managed by a multidisciplinary approach. Treatment considerations include the patient's age, status of skeletal growth and severity of tooth agenesis and morphological abnormalities, and psychological status. Treatment options are removable dentures, toothsupported fixed partial dentures and implant supported prostheses.
Imaging plays an important role in planning and monitoring of the treatment. Given that many of these treatments are initiated in early childhood, prosthetic restoration is complicated by the ongoing skeletal growth and remodeling. For example, placement of implants early in life is complicated by the continual tooth eruption coupled with the growth and development of the jaws, which result in alterations in the vertical dimension and shifts in the occlusion. This may result in implant submergence or an open bite. Typically, growth of the anterior mandible is completed by approximately 10-12 years of age. Thus, implant placement in the anterior mandible at this age is an option. However, the mandibular body and ramus continue to grow until early adulthood. Skeletal growth assessment, as with hand-wrist radiographs is of importance to plan timing of implant placement. Furthermore, orthodontic tooth movement to optimally position the teeth for implant-supported prostheses or tooth-supported partial dentures is often required.
Cone beam CT provides crucial information on the height and width of the alveolar ridges, allows for assessment of bone quality at potential implant sites and evaluation of the need for possible bone augmentation procedures. Given the diagnostic task and the area to be imaged, this may be accomplished by limited- or medium-field of view CBCT. Additionally, patients with Xlinked hypohidrotic ED demonstrate increased mineralized of the trabecular bone, especially in the anterior mandible, and this may potentially compromise implant osseointegration.
The 2 cases shown here demonstrate the value of CBCT imaging in treatment planning of patients with oligodontia manifesting in ED.
Imaging plays an important role in planning and monitoring of the treatment. Given that many of these treatments are initiated in early childhood, prosthetic restoration is complicated by the ongoing skeletal growth and remodeling. For example, placement of implants early in life is complicated by the continual tooth eruption coupled with the growth and development of the jaws, which result in alterations in the vertical dimension and shifts in the occlusion. This may result in implant submergence or an open bite. Typically, growth of the anterior mandible is completed by approximately 10-12 years of age. Thus, implant placement in the anterior mandible at this age is an option. However, the mandibular body and ramus continue to grow until early adulthood. Skeletal growth assessment, as with hand-wrist radiographs is of importance to plan timing of implant placement. Furthermore, orthodontic tooth movement to optimally position the teeth for implant-supported prostheses or tooth-supported partial dentures is often required.
Cone beam CT provides crucial information on the height and width of the alveolar ridges, allows for assessment of bone quality at potential implant sites and evaluation of the need for possible bone augmentation procedures. Given the diagnostic task and the area to be imaged, this may be accomplished by limited- or medium-field of view CBCT. Additionally, patients with Xlinked hypohidrotic ED demonstrate increased mineralized of the trabecular bone, especially in the anterior mandible, and this may potentially compromise implant osseointegration.
The 2 cases shown here demonstrate the value of CBCT imaging in treatment planning of patients with oligodontia manifesting in ED.
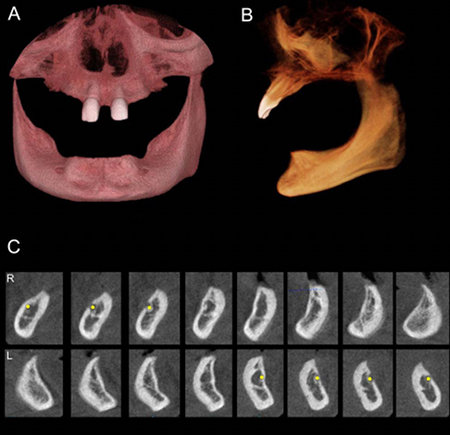
Fig. 1: CBCT images of a 10-year-old male with ED. The examination was done to evaluate the jaws for implant-supported overdentures. Implant placement was planned in the mandibular canine regions. CBCT images were acquired in a 6-inch field of view.
A and B: 3D volume renderings demonstrate almost complete absence of the permanent dentition. Only the maxillary central incisors are present. Edentulous ridges of the maxilla and mandible are markedly atrophic.
C: Selected cross-sectional slices of the mandibular anterior and premolar region. Note atrophic, knife-edged ridge especially in the midline. Buccal and lingual plates are well corticated and the trabecular bone density appears adequate for implant placement.
A and B: 3D volume renderings demonstrate almost complete absence of the permanent dentition. Only the maxillary central incisors are present. Edentulous ridges of the maxilla and mandible are markedly atrophic.
C: Selected cross-sectional slices of the mandibular anterior and premolar region. Note atrophic, knife-edged ridge especially in the midline. Buccal and lingual plates are well corticated and the trabecular bone density appears adequate for implant placement.
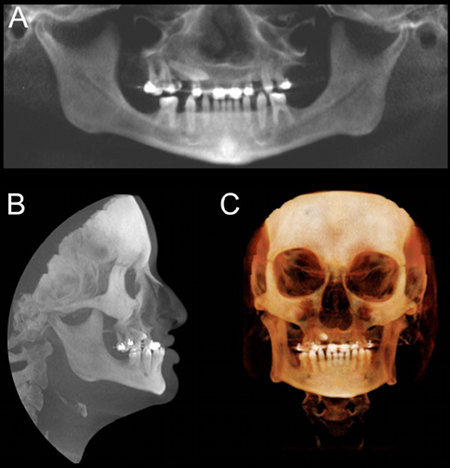
Fig. 2: A 20-year old male patient with ED referred for CBCT imaging for orthodontic assessment and for potential implant treatment planning. The CBCT examination was done using a 12-inch field of view.
A: Panoramic reconstruction showing oligodontia. The maxillary right canine is impacted. Also note multiple conical-shaped crowns.
B: A maximum-intensity projection (MIP) demonstrating a hypoplastic maxilla and slightly prognathic mandible.
C: 3-D volume rendering
A: Panoramic reconstruction showing oligodontia. The maxillary right canine is impacted. Also note multiple conical-shaped crowns.
B: A maximum-intensity projection (MIP) demonstrating a hypoplastic maxilla and slightly prognathic mandible.
C: 3-D volume rendering
REFERENCES
White SC, Pharoah MJ. Oral radiology : principles and interpretation. 6th edn. St. Louis, Mo.: Mosby/ Elsevier, 2009. Pages 295-298.
Pub Med Health: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002440/
Pub Med Health: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002440/