
Quality Dental Radiology In Italy:
|






|

It goes through a review of the continuing education of professionals involved, since their first work assignment: need for better planning of courses relevant to the real training needs of each professional.
Then serve interdisciplinary meetings involving the dental clinic, the radiologist and technologist, to stimulate greater collaboration by exploiting correct and commensurate with the potential and the real needs of all new diagnostic technology.
The exponential growth of demand for radiological investigation in dentistry involves professional development for all professionals involved, on both ethical and professional and legally, to address the growing problems related to medical-legal professional liability.
Through a survey, which involved three professionals (radiographers and Dentists in Italy and Dentists radiology technicians in the U.S.) we tried to find gaps in the technical quality of the most popular methods in radiology Oral (Orthopantomography, cephalometric skull, by CT study of the dental arches) and have proposed solutions that will help to improve the quality of our product and then going to increase the efficiency of service while minimizing errors and reducing costs.
The comparison with American colleagues is very important to understand the level of technology and skills that we seek. Should be taken into account that in Italy the majority of radiology are public and dentists are private.In Italy, most dentists do not have equipment radiological studies and exams are performed at public facilities.
Data quality is considered good in view of the fact that in Italy come from different regions and almost never (1 case) from the same body of membership.
From the questionnaires we can extrapolate some interesting considerations.
1) The quality of the images offered to dentists is enough? The dentists say yes for 27% but 63% said yes and no. The reason for this uncertainty is partly due to the technology used (we are still in a transition phase analog-digital and those who have embraced the digital to analog back trouble) reasons both technical implementation which is worth reflecting on. Of course, digital technology is by far preferred (82%) to analog as it allows the dentist to easily perform the post-processing (82%) and consequently to reduce errors of over-under exposure typical radiographic image analog.
2) The majority of dentists surveyed (45%) say that about 10% of tests are performed inappropriately. If we compare this figure with that given by the technicians (8% say they are not satisfied with the quality of images that give to the patient) we find that both groups agree that there is something that does not work and which would be right to intervene.
3) The majority of both categories of professionals say they are in favor of meetings to discuss technical issues that help solve problems. Currently, however, the two categories are quite detached fact that 88% of the technicians say they have no professional relationship for the exchange of ideas with dentists.
4) For the main errors in radiographic dental examination, both professions recognize the imperfect positioning of the patient (hyperipoflessione and asymmetry of the head) and occlusion incorrect. Decrease exposure errors due to the use of digital systems. Do not underestimate the problems due to the use of digital systems: problems related to the views of digital media (27% of the dentists have trouble opening the CD) and problems with correct interpretation of measurements of magnification and reference data (18 % of dentists).
5) Regarding the technology used, we are now in an almost complete transition to digital even though there is still 24% of the technicians using an analog system with a film and only 1% use of Cone Beam CT systems. Interesting in this case is the comparison with their American counterparts where no one makes more use of analogue and as much as 76% use the Cone Beam CT.
6) A proposal to improve the professional performance of technologists can be deduced from the analysis of the last part of the questionnaires in which they are taken into account the technical knowledge possessed by, the development of professional skills and the period of coaching to a professional. The first finding is that all the engineers, before work, had specific knowledge (anatomy and protectionist) to perform examinations and dental x-rays-a good percentage (44%), including knowledge of equipment. Interestingly, the subsequent development of skills. For the majority of the technicians need at least a month to run a test and TC OPT to a patient with dental problems and to recognize all the technical problems and at least two months to be able to find all the solutions themselves. Roughly the same percentages were extrapolated from the questionnaires delivered to technicians in the U.S.. In the face of so long time needed to achieve specific skills is echoed in the actual timing of the reserves for each business coaching hires: 95% say they opt for 1 week and 64% said 1 week for TC. Situation a little 'different in the U.S. where 61% said 1 month for OPT, and 46% said 2 months for TC. The proposal is best to develop a project that allows the new employee to acquire a gradual increase in skills is not autonomous but accompanied and supervised by experienced staff for a period not too short as that of a week.
The analysis of expert professional skills, ie ability to produce quality tests and the ability to identify errors and remove them, a survey was conducted with images stored on PACS archive. 100 images have been taken out of OPT, 100 of skull X-rays and 50 CT Dentalscan. The images were viewed separately, by a student technologists to 3 rd year and a technician with proven experience.
It is evident the difference in ability to analyze errors, particularly in methods such as CT, which requires experience and specific skills. Here the student is unable to find errors as the technical expert examinations found a 6% deficient in quality.
Even in the simple tests that can seem like the OPT or cephalometric, the technical expert, unlike the student fails to detect a good percentage of errors to be avoided and that only a fair job experience allows us to identify and possibly limit.
Problems that emerged from the study:
QUESTIONNAIRE
Dear Colleague, this questionnaire is a invitation to participate in a research study on the topic dental arches in radiology: studying the technical issues in relation to the needs of the medical practitioner.
The questionnaire is anonymous and no reference to property or person will be reported in the statistical data obtained. The data will be used solely for the preparation of a thesis in medical radiology.
To all of you from AADMRT I would like to thank you for your cooperation.
QUESTION 1
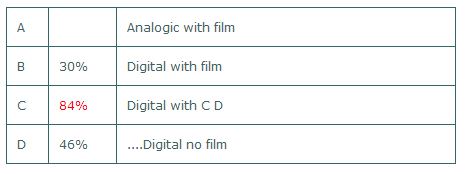
Among the technologies used in the reproduction of a radiological study of the dental arches, you use:
Then serve interdisciplinary meetings involving the dental clinic, the radiologist and technologist, to stimulate greater collaboration by exploiting correct and commensurate with the potential and the real needs of all new diagnostic technology.
The exponential growth of demand for radiological investigation in dentistry involves professional development for all professionals involved, on both ethical and professional and legally, to address the growing problems related to medical-legal professional liability.
Through a survey, which involved three professionals (radiographers and Dentists in Italy and Dentists radiology technicians in the U.S.) we tried to find gaps in the technical quality of the most popular methods in radiology Oral (Orthopantomography, cephalometric skull, by CT study of the dental arches) and have proposed solutions that will help to improve the quality of our product and then going to increase the efficiency of service while minimizing errors and reducing costs.
The comparison with American colleagues is very important to understand the level of technology and skills that we seek. Should be taken into account that in Italy the majority of radiology are public and dentists are private.In Italy, most dentists do not have equipment radiological studies and exams are performed at public facilities.
Data quality is considered good in view of the fact that in Italy come from different regions and almost never (1 case) from the same body of membership.
From the questionnaires we can extrapolate some interesting considerations.
1) The quality of the images offered to dentists is enough? The dentists say yes for 27% but 63% said yes and no. The reason for this uncertainty is partly due to the technology used (we are still in a transition phase analog-digital and those who have embraced the digital to analog back trouble) reasons both technical implementation which is worth reflecting on. Of course, digital technology is by far preferred (82%) to analog as it allows the dentist to easily perform the post-processing (82%) and consequently to reduce errors of over-under exposure typical radiographic image analog.
2) The majority of dentists surveyed (45%) say that about 10% of tests are performed inappropriately. If we compare this figure with that given by the technicians (8% say they are not satisfied with the quality of images that give to the patient) we find that both groups agree that there is something that does not work and which would be right to intervene.
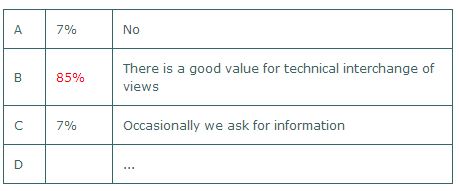
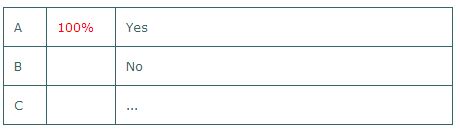
3) The majority of both categories of professionals say they are in favor of meetings to discuss technical issues that help solve problems. Currently, however, the two categories are quite detached fact that 88% of the technicians say they have no professional relationship for the exchange of ideas with dentists.
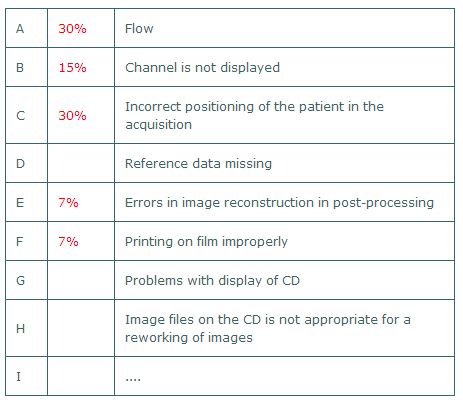
4) For the main errors in radiographic dental examination, both professions recognize the imperfect positioning of the patient (hyperipoflessione and asymmetry of the head) and occlusion incorrect. Decrease exposure errors due to the use of digital systems. Do not underestimate the problems due to the use of digital systems: problems related to the views of digital media (27% of the dentists have trouble opening the CD) and problems with correct interpretation of measurements of magnification and reference data (18 % of dentists).
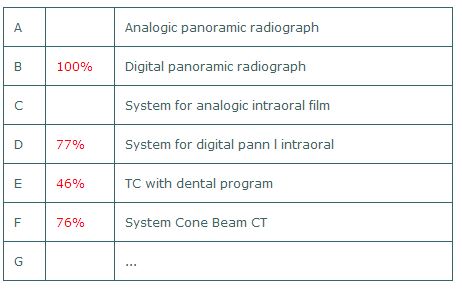
5) Regarding the technology used, we are now in an almost complete transition to digital even though there is still 24% of the technicians using an analog system with a film and only 1% use of Cone Beam CT systems. Interesting in this case is the comparison with their American counterparts where no one makes more use of analogue and as much as 76% use the Cone Beam CT.
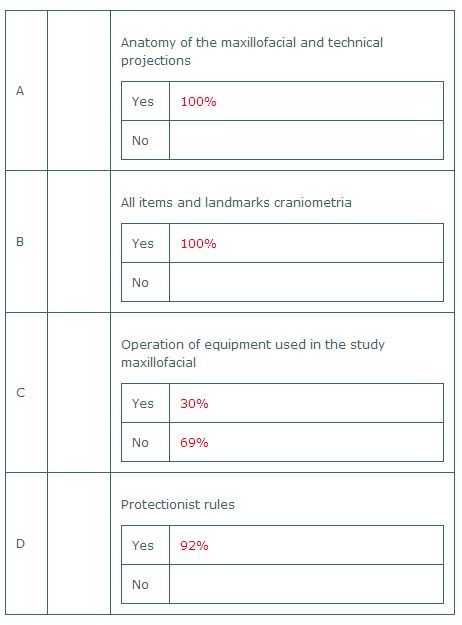
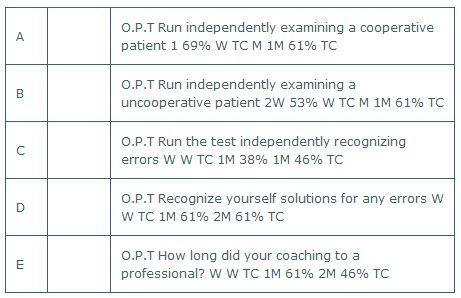
6) A proposal to improve the professional performance of technologists can be deduced from the analysis of the last part of the questionnaires in which they are taken into account the technical knowledge possessed by, the development of professional skills and the period of coaching to a professional. The first finding is that all the engineers, before work, had specific knowledge (anatomy and protectionist) to perform examinations and dental x-rays-a good percentage (44%), including knowledge of equipment. Interestingly, the subsequent development of skills. For the majority of the technicians need at least a month to run a test and TC OPT to a patient with dental problems and to recognize all the technical problems and at least two months to be able to find all the solutions themselves. Roughly the same percentages were extrapolated from the questionnaires delivered to technicians in the U.S.. In the face of so long time needed to achieve specific skills is echoed in the actual timing of the reserves for each business coaching hires: 95% say they opt for 1 week and 64% said 1 week for TC. Situation a little 'different in the U.S. where 61% said 1 month for OPT, and 46% said 2 months for TC. The proposal is best to develop a project that allows the new employee to acquire a gradual increase in skills is not autonomous but accompanied and supervised by experienced staff for a period not too short as that of a week.
The analysis of expert professional skills, ie ability to produce quality tests and the ability to identify errors and remove them, a survey was conducted with images stored on PACS archive. 100 images have been taken out of OPT, 100 of skull X-rays and 50 CT Dentalscan. The images were viewed separately, by a student technologists to 3 rd year and a technician with proven experience.
It is evident the difference in ability to analyze errors, particularly in methods such as CT, which requires experience and specific skills. Here the student is unable to find errors as the technical expert examinations found a 6% deficient in quality.
Even in the simple tests that can seem like the OPT or cephalometric, the technical expert, unlike the student fails to detect a good percentage of errors to be avoided and that only a fair job experience allows us to identify and possibly limit.
Problems that emerged from the study:
- Dissatisfaction by those still using analogue systems
- Period of coaching too short
- Lack of collaboration between dentists / technologists / radiologists
- Lack of latest technology: CTCB.
- Training: accurate basic computer training for all staff and targeted training based on the needs of each.
- Training of hires: will be drawn up a detailed protocol for the coaching of new hires that lasts at least 1-2 months and allowing the new employee to mature, passing easily from one level to a novice to expert.
- Organize interdisciplinary meetings: will start a series of meetings between the three professions in order to bring the three skills to solve simple and complex problems and a continuous exchange of ideas and information.
QUESTIONNAIRE
Dear Colleague, this questionnaire is a invitation to participate in a research study on the topic dental arches in radiology: studying the technical issues in relation to the needs of the medical practitioner.
The questionnaire is anonymous and no reference to property or person will be reported in the statistical data obtained. The data will be used solely for the preparation of a thesis in medical radiology.
To all of you from AADMRT I would like to thank you for your cooperation.
QUESTION 1
Among the technologies used in the reproduction of a radiological study of the dental arches, you use:
QUESTION 2
Where you work, what kind of machines are there?
Where you work, what kind of machines are there?
QUESTION 3
You or your coordinator have a technical exchange of views with dental clinics?
You or your coordinator have a technical exchange of views with dental clinics?
QUESTION 4
Do you think it would be useful to periodically compare staff technologist / dentists to assess technical issues and procedures ?
Do you think it would be useful to periodically compare staff technologist / dentists to assess technical issues and procedures ?
QUESTION 5
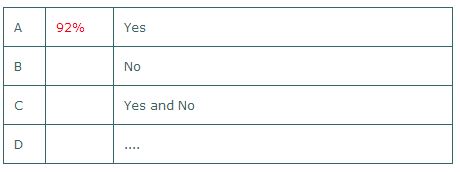
Are you satisfied with the technical quality of examinations that deliver to patients?
Are you satisfied with the technical quality of examinations that deliver to patients?
QUESTION 6
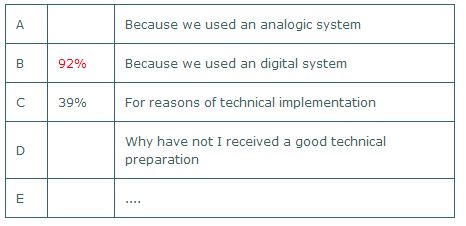
The previous response is due to:
The previous response is due to:
QUESTION 7
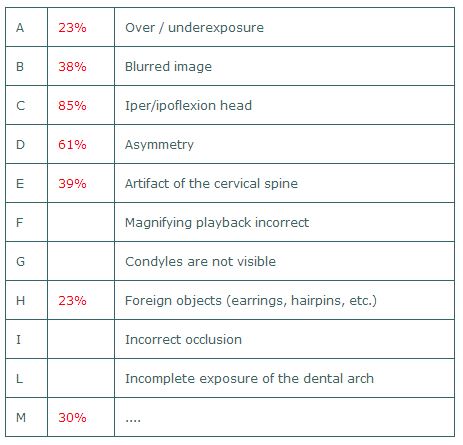
Here are a number of technical errors for three types of examinations. Indicate the three mistakes that you think are most common.
In the panoramic radiograph (O.P.T.):
Here are a number of technical errors for three types of examinations. Indicate the three mistakes that you think are most common.
In the panoramic radiograph (O.P.T.):
In Teleradiography:
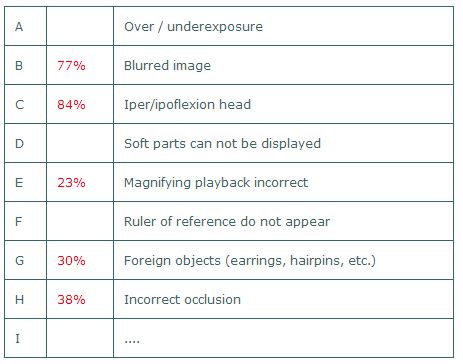
In TC Dental
QUESTION 8
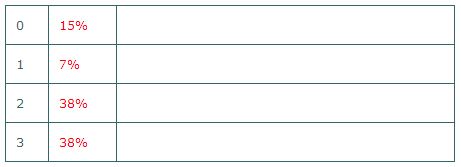
Over the past five years, how many training courses in the field of dental radiology attended?
Over the past five years, how many training courses in the field of dental radiology attended?
QUESTION 9
Think for a moment in the first period of your career and what has lasted its full learning techniques applied to dental radiology. Before starting your career you had all this knowledge?
Think for a moment in the first period of your career and what has lasted its full learning techniques applied to dental radiology. Before starting your career you had all this knowledge?
And from the first day you was assigned to this type of test, how long it took to reach an expert competence? For each of the following (with numbers, indicate the duration, ex. 1-2 next to W and M, respectively, which indicate the week and month):
T.S.R.M. Sandro, Dr. Gasparato
Noventa Vicentinia (Vicenza-Italy)
Technical Diploma in Medical radiology a the Hospital of Padua.
Degree in Medical Radiology techniques Imaging and Radiotherapy Unniverity G.D.'Annunzio-Chieti with vote 110/110.
Coordination Master in Health Professions-Unitelma/Sapienza/University of rome with vote 110/110.
Since 2006 Student Internship Guide TSRM University of Padua.
Work with a qualified technologist Radiology at the Public Hospital of Noventa Vicentina (ULSS 6-Vicenza)
Also:
Diploma in mammographc technique and quality control-Italian School of breast and 86 refresher courses
Technical guide in 4 thesis
Noventa Vicentinia (Vicenza-Italy)
Technical Diploma in Medical radiology a the Hospital of Padua.
Degree in Medical Radiology techniques Imaging and Radiotherapy Unniverity G.D.'Annunzio-Chieti with vote 110/110.
Coordination Master in Health Professions-Unitelma/Sapienza/University of rome with vote 110/110.
Since 2006 Student Internship Guide TSRM University of Padua.
Work with a qualified technologist Radiology at the Public Hospital of Noventa Vicentina (ULSS 6-Vicenza)
Also:
Diploma in mammographc technique and quality control-Italian School of breast and 86 refresher courses
Technical guide in 4 thesis