
Use of Tomography For Evaluating Impacted Posterior TeethDr. Kenneth Abramovitch
Associate Professor of Oral and Maxillofacial Radiology Dental Branch, University of Texas Health Science Center, Houston Texas From the Spring 2003 AADMRT Newsletter  Dr. Kenneth Abramovitch Dr. Kenneth Abramovitch
Imaging impacted teeth is a frequently requested diagnostic task for multiple dental disciplines including oral and maxillofacial radiologists, surgeons and pathologists. In addition to the conventional intraoral and panoramic images, more advanced imaging techniques may become necessary to access impacted teeth in the posterior arches. The images are necessary due to the various treatment protocols that exist for managing impacted teeth. Potential management decisions include extraction, movement or serial observation.
The criteria for imaging impacted teeth include identifying the impactions within the confines of the surrounding alveolar bone, then to determine their location relative to adjacent teeth and vital structures in the dento-alveolar complex and then finally to evaluate whether there is pathology that is affecting adjacent tissues. Even without pathology present, the images are still beneficial in determining the potential morbidity and prognosis of an impacted tooth. Once the diagnostic (i.e, radiographic and clinical) information is obtained, a treatment decision can be made more confidently. If surgery is indicated, then precise location and proximity to vital structures (i.e., air spaces, neurovascular canals, etc...) is again reviewed to establish the surgical treatment plan. Multi-plane views help yield the clinical perspective necessary for such treatment planning decisions. The concept of using multiple-angle radiographic projections to more precisely image structures in the dento-alveolar complex is not a new imaging concept. In 1910, Clark's description of the use of multiple images to localize unerupted teeth was published in the Odontologic Section of the Proceedings of the Royal Society of Medicine.1 Albert Richards further supported and documented this principle for localization of impacted third molars2 and for localization of the mandibular canal.3 Other reports of more recent vintage have summarized these techniques.4,5 The advent of multitask imaging (x-ray) units has provided additional armamentarium and techniques for evaluating impacted teeth. These units can support several types of complex motion, therefore various imaging techniques ranging from rotational panoramic radiography to complex motion plain film tomography are possible. Previous articles presented the utility of cross-sectional tomographic images of the mandibular dental arch for demonstrating the location of the mandibular nerve adjacent impacted third molars.6,7 The cross-sectional tomographic imaging technique continues to serve as a beneficial imaging modality to establish a surgical treatment plan and then to guide the surgical access. This review article will present five cases where the use of cross-sectional imaging of the jaws has been helpful in evaluating impacted teeth in the posterior maxillary and mandibular dental archs. |






|
Case 1
A panoramic radiograph helps to evaluate the degree of impaction of the right mandibular second molar (Figure 1). The patient is a 21 year-old male. The impacted second molar has a 3-4.0mm wide follicular sac. This widened pericoronal radiolucency attaches at the cementoenamel junction and does not extend apically along the root surface. Within the radiolucent lumen, there is an amorphous radiopacity, approximately 2 mm by 6 mm in greatest dimensions that rests adjacent the distal occlusal surface of the crown. The rarefaction of the adjacent trabecular bone is from the abscessed first molar. The degree of inferior impaction has caused prominent displacement of the inferior alveolar canal (i.e., IAC). Since the IAC and the apical half of the root are superimposed, it is not possible to determine the relative positions of these structures to each other. From Figure 2, the IAC is lingually positioned and appears to be slotted between the impaction and the inferior-lingual mandibular cortex. Surprisingly, the patient did not report symptoms of parasthesia. The degree of impaction and the identification of a mineralization in the follicular space were radiographic signs suspicious for an odontogenic tumor or cyst. Surgery was planned. During surgery, the roots of the impacted second molar had to be sectioned to maintain continuity and avoid damage to the mandibular nerve. Normal nerve sensation returned within two weeks of the surgery.
A panoramic radiograph helps to evaluate the degree of impaction of the right mandibular second molar (Figure 1). The patient is a 21 year-old male. The impacted second molar has a 3-4.0mm wide follicular sac. This widened pericoronal radiolucency attaches at the cementoenamel junction and does not extend apically along the root surface. Within the radiolucent lumen, there is an amorphous radiopacity, approximately 2 mm by 6 mm in greatest dimensions that rests adjacent the distal occlusal surface of the crown. The rarefaction of the adjacent trabecular bone is from the abscessed first molar. The degree of inferior impaction has caused prominent displacement of the inferior alveolar canal (i.e., IAC). Since the IAC and the apical half of the root are superimposed, it is not possible to determine the relative positions of these structures to each other. From Figure 2, the IAC is lingually positioned and appears to be slotted between the impaction and the inferior-lingual mandibular cortex. Surprisingly, the patient did not report symptoms of parasthesia. The degree of impaction and the identification of a mineralization in the follicular space were radiographic signs suspicious for an odontogenic tumor or cyst. Surgery was planned. During surgery, the roots of the impacted second molar had to be sectioned to maintain continuity and avoid damage to the mandibular nerve. Normal nerve sensation returned within two weeks of the surgery.

Figure 1: The horizontally impacted second molar has also displaced the IAC. Note the mineralization within the follicular space of the molar (see arrow). Root canal therapy has just been completed to treat the dental abscess on the first molar.
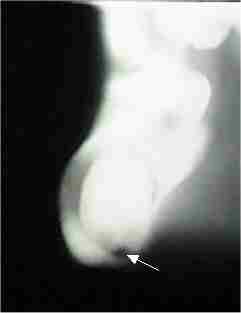
Figure 2: The arrow shows the inferiorly and lingually displaced IAC on the cross-sectional tomograms. Rarefaction of the buccal trabecular bone from the dental abscess is also noted.
The histologic diagnosis was a calcified epithelial odontogenic tumor (i.e., Pindborg tumor). Although Pindborg tumor metastases have been reported,3 these lesions generally spread by direct extension. Surgeries can range from enucleation as in this case, to resection depending on the degree of invasion. The recurrence rate is 20%, therefore most of these lesions do not require the aggressive surgeries necessary for more potentially destructive lesions such as the ameloblastoma and certain types of odontogenic keratocysts.
Case 2
This 47 year-old male was being evaluated for orthodontic treatment. There is an impacted mandibular supernumerary tooth in the left mandible (Figure 3). The location of the impaction presents as an obstruction to the proper orthodontic alignment of the mandibular teeth. Consequently, extraction of this supernumerary tooth is necessary. Precise location of the impacted tooth's roots relative to the first molar is important to determine the surgical access.
Case 2
This 47 year-old male was being evaluated for orthodontic treatment. There is an impacted mandibular supernumerary tooth in the left mandible (Figure 3). The location of the impaction presents as an obstruction to the proper orthodontic alignment of the mandibular teeth. Consequently, extraction of this supernumerary tooth is necessary. Precise location of the impacted tooth's roots relative to the first molar is important to determine the surgical access.

Figure 3: The position of the impacted mandibular premolar will complicate the impending orthodontic treatment.
The cross-sectional tomograms (Figure 4) demonstrate that the roots of the supernumerary tooth roots are lingual to the molar roots. Also note the expansion and thinning of the lingual cortex from the position of the supernumerary tooth's roots. One can also see that the IAC is approximately 10 mm. inferior to the impaction.

Figure 4: The roots of the impacted premolar are lingually positioned and are also causing expansion of the lingual cortical bone.
Case 3
This 45 year-old female was considering root form dental implants in the right mandible as a possible restorative treatment planning option. However, an impacted premolar has complicated this restorative treatment option (Figure 5). The position of the impacted tooth is superimposing the anterior IAC and the mental foramen. The cross-sectional tomograms in Figure 6 demonstrate the lingual position of the impaction relative to the IAC and mental foramen. The follicular space is within normal limits and there is no pathology associated with the impaction. Due to the position of the impaction and the high position of the IAC in the edentulous ridge, surgical removal of the tooth would further reduce the size of the already atrophic ridge. The best treatment option at this time would be to leave the impaction, and serially observe it over time. Based on this radiographic evaluation, root form implants are not a viable restorative treatment option at this time.
This 45 year-old female was considering root form dental implants in the right mandible as a possible restorative treatment planning option. However, an impacted premolar has complicated this restorative treatment option (Figure 5). The position of the impacted tooth is superimposing the anterior IAC and the mental foramen. The cross-sectional tomograms in Figure 6 demonstrate the lingual position of the impaction relative to the IAC and mental foramen. The follicular space is within normal limits and there is no pathology associated with the impaction. Due to the position of the impaction and the high position of the IAC in the edentulous ridge, surgical removal of the tooth would further reduce the size of the already atrophic ridge. The best treatment option at this time would be to leave the impaction, and serially observe it over time. Based on this radiographic evaluation, root form implants are not a viable restorative treatment option at this time.

Figure 5: The impacted premolar is superimposing the mental foramen and the IAC.
|

Figure 6: With the benefit of the cross-sectional tomograms, the mental foramen and the IAC are identified buccal to the impaction.
|
Case 4
This 9 year male was undergoing orthodontic treatment. Radiographs were taken to determine a cause for the delayed eruption of the maxillary right second premolar. A permanent successor is not present in the periapical region of deciduous tooth "A" (Figure 7). There is a blurred radiopacity in the periapical region of the first molar, i.e., #3. Since this radiopacity is wide and lacks sharp resolution, there is a suspicion that this may be the second premolar displaced posteriorly and toward the palate. Consequently, there is difficulty with the panoramic image being able to demonstrate structures located outside of the panoramic focal trough. From the cross-sectional image (Figure 8), the vertically impacted second premolar is easily identified, thus ruling out other sources of pathology. Based on these images, the orthodontic treatment can be modified. The second premolar can be ligated and then orthodontic forces can be applied to guide the premolar to its proper arch position.
This 9 year male was undergoing orthodontic treatment. Radiographs were taken to determine a cause for the delayed eruption of the maxillary right second premolar. A permanent successor is not present in the periapical region of deciduous tooth "A" (Figure 7). There is a blurred radiopacity in the periapical region of the first molar, i.e., #3. Since this radiopacity is wide and lacks sharp resolution, there is a suspicion that this may be the second premolar displaced posteriorly and toward the palate. Consequently, there is difficulty with the panoramic image being able to demonstrate structures located outside of the panoramic focal trough. From the cross-sectional image (Figure 8), the vertically impacted second premolar is easily identified, thus ruling out other sources of pathology. Based on these images, the orthodontic treatment can be modified. The second premolar can be ligated and then orthodontic forces can be applied to guide the premolar to its proper arch position.
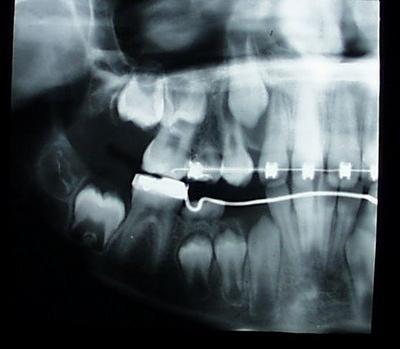
Figure 7: A wide, blurred radiopacity is noted periapical to tooth #3. The permanent second premolar is not in its usual position periapical to the second deciduous molar, tooth "A".
|

Figure 8: The cross-sectional image demonstrates the position of the permanent second premolar. It is vertically impacted in the alveolar bone palatal to the first molar.
|
Case 5
This sixteen year-old male has congenital maxillary hypoplasia. The underdevelopment of the maxilla has caused malocclusion of the dentition and impaction of the maxillary molars. As was discussed in Case 4, palatal structures impacted toward the midline are often distorted on panoramic images as they are further from the panoramic focal trough. They may also distort from the orthogonal projection geometry of the x-ray beam. The panoramic image in Figure 9 demonstrates the molar impactions in the left maxilla. However, based on the panoramic distortion, the structure posterior to the left second molar has the appearance of a mineralized tumor; perhaps a complex odontoma. The cross-sectional tomograms (Figure 10) provide images with minimal geometric distortion. The angle of beam projection also better demonstrates the structure and the outline of a normally developing third molar. Although surgery is required to remove the impactions, the surgical access can be more conservative than it would be for irregular shaped or more aggressive tumors.
This sixteen year-old male has congenital maxillary hypoplasia. The underdevelopment of the maxilla has caused malocclusion of the dentition and impaction of the maxillary molars. As was discussed in Case 4, palatal structures impacted toward the midline are often distorted on panoramic images as they are further from the panoramic focal trough. They may also distort from the orthogonal projection geometry of the x-ray beam. The panoramic image in Figure 9 demonstrates the molar impactions in the left maxilla. However, based on the panoramic distortion, the structure posterior to the left second molar has the appearance of a mineralized tumor; perhaps a complex odontoma. The cross-sectional tomograms (Figure 10) provide images with minimal geometric distortion. The angle of beam projection also better demonstrates the structure and the outline of a normally developing third molar. Although surgery is required to remove the impactions, the surgical access can be more conservative than it would be for irregular shaped or more aggressive tumors.

Figure 9: The second molar is vertically impacted in the posterior maxilla. From this panoramic projection, there appears to be a complex odontoma or related mineralized tumor causing the impaction.
|

Figure 10: The cross-sectional image projections provide better views that confirm that there is a normally developing third molar. These impactions appear to be solely related to maxillary hypo-plasia.
|
Summary
The following three mandibular and two maxillary cases demonstrate how cross-sectional tomography can assist the radiographic diagnosis and contribute to the formulation of both surgical and orthodontic treatment plans. These cross-sectional tomographic images are readily obtained with multi-task x-ray machines. Knowledge of the specific program modalities on these machines is readily applicable to the generation of useful images. These images can then contribute to a patient's radiographic diagnosis and then ultimately to their treatment plans.
The following three mandibular and two maxillary cases demonstrate how cross-sectional tomography can assist the radiographic diagnosis and contribute to the formulation of both surgical and orthodontic treatment plans. These cross-sectional tomographic images are readily obtained with multi-task x-ray machines. Knowledge of the specific program modalities on these machines is readily applicable to the generation of useful images. These images can then contribute to a patient's radiographic diagnosis and then ultimately to their treatment plans.
REFERENCES
- Clark, CA. A method of ascertaining the relative position of unerupted teeth by means of film radiographs. Odont Sec Roy Soc Med Proc 3:87-90, 1909-1910.
- Richards, AG. A technic for the roentgenographic examination of impacted mandibular third molars. J Oral Surg 10:138-141, 1952.
- Richards, AG. Radiographic localization of the mandibular canal. J Oral Surg 10:325-329, 1952.
- Langlais, RP, Langland, OE, Morris, CR. Radiographic localization technics. Dent Radiog Photog 52(4):69-77, 1979.
- Abramovitch, K. Imagery. Chapter 5, In Alling, CC, Helfrick, JF, Alling, RD. Impacted Teeth, Saunders, Philadelphia, 1993. pp. 97-123.
- Miller, CS, Nummikoski, PV, Barnett, DA, Langlais, RP. Cross-sectional tomography. A diagnostic technique for determining the buccolingual relationship of impacted mandibular third molars and the inferior alveolar neurovascular bundle. Oral Surg Oral Med Oral Pathol 70:791-797, 1990.
- Abramovitch, K. Tomographic localization of the mandibular nerve adjacent to impacted third molars. Contemporary Esthetics and Restorative Practice, 42-47,2000.
About the Author:
Dr. Kenneth Abramovitch is an Associate Professor of Oral and Maxillofacial Radiology at the Dental Branch of the University of Texas Health Science Center at Houston. He maintains a private practice in oral and maxillofacial radiology and oral medicine in Houston Texas.
Although a member of several professional societies, associations and academies, Dr. Abramovitch is currently President-Elect of the American Academy of Oral and Maxillofacial Radiology. Among other scholarly pursuits, he is a Diplomate of the American Board of Oral and Maxillofacial Radiology and a Diplomate of the American Board of Oral Medicine.