
Surgically Assisted Palate Expand for a Full Braces
|

Dr. Lee Mettler
|
As the years go by, our office gets the opportunity to retreat young adult patients who received braces treatment during their preteen and teenage years. This article is a case presentation for a patient who was treated twelve years earlier with full braces treatment with the removal of the four first pre molars, then treated again years later.
|
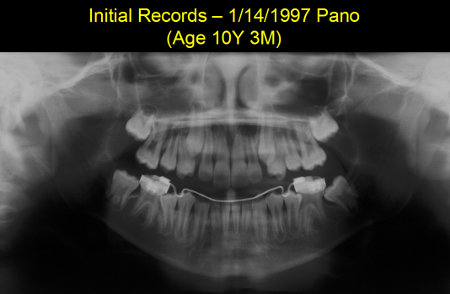
Figure 1: Initial Records - 1/14/1997 Pano (Age 10Y 3M)
Figure 1 is an Initial Records Pano taken on 1/14/1997 when our patient was 10Y, 3M of age. This Pano shows the lower left 2nd molar and both lower 2nd premolar with insufficient space in the arch for full eruption.
Figure 2 is identified as Final Records (Final Models) at age 14Y, 8M. Our patient was dismissed from scheduled appointments with instructions to wear her removable upper retainer at night. The lower teeth were held in their treated position by a bonded, lingual retainer.
Figure 1 is an Initial Records Pano taken on 1/14/1997 when our patient was 10Y, 3M of age. This Pano shows the lower left 2nd molar and both lower 2nd premolar with insufficient space in the arch for full eruption.
Figure 2 is identified as Final Records (Final Models) at age 14Y, 8M. Our patient was dismissed from scheduled appointments with instructions to wear her removable upper retainer at night. The lower teeth were held in their treated position by a bonded, lingual retainer.






Figure 2: Final Records-5/14/2001 (Age 14Y,8M)
|

Figure 3: Post Final-11/11/2008 (Age 22Y,2M)
|
Seven and one half years later after the date of the final models the patient presented with a clinical condition shown above in figure 3. Her Clinical condition as shown is described as a Class III malocclusion with unilateral upper posterior teeth lingual crossbites (on the left side) and a severe midline discrepancy of 3 to 4 millimeters.
After consultations with Oral Surgeons and the parents, the treatment plan including surgically-assisted palatal expansion and nonsurgical, orthodontic correction of the Class III malocclusion was agreed upon.
After consultations with Oral Surgeons and the parents, the treatment plan including surgically-assisted palatal expansion and nonsurgical, orthodontic correction of the Class III malocclusion was agreed upon.
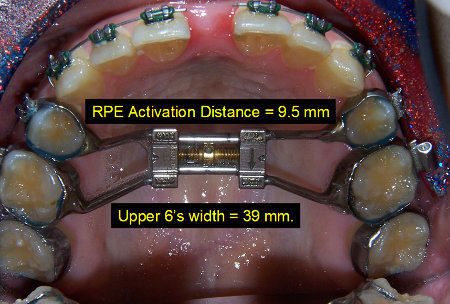
Figure 4: Progress Records (3) 1-19-2009
Figure 4 dated 1/19/2009 shows the maxillary arch occlusal view after surgically assisted palatal expansion. The large upper midline space reflects a successful separation of the two halves of the maxilla. The surgical procedure was completed on 12/24/2008.

Figure 5
Figure 5 is the frontal photo of the upper and lower teeth showing the large upper midline space on 1/19/2009. Her midline space was measured at 6 millimeters at this time.
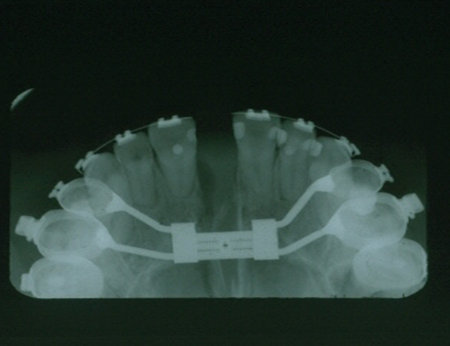
A Progress Pano was taken on the same day as the previous photos and is shown in Figure 6.
A Progress Pano was taken on the same day as the previous photos and is shown in Figure 6.

Figure 6
The occlusal views shown in Figure 7 taken on the same 1/19/2009 show how the appliance center area is expanded to the maximum advisable by the manufacturer. This represents about one month post-surgery.

|
|
Figure 7: Two Upper Occlusal Views 1/19/2009
Over the next two months we observed a steady and (surprising) complete closing of the midline space with no orthodontic force applied - it's the stretch created in the gingival fibers by the expansion process that pulls the teeth together. Note the new and persistent midline discrepancy seen at Figure 8.
Over the next two months we observed a steady and (surprising) complete closing of the midline space with no orthodontic force applied - it's the stretch created in the gingival fibers by the expansion process that pulls the teeth together. Note the new and persistent midline discrepancy seen at Figure 8.

Figure 8: The central incisors are edge-to-edge

Figure 9
The occlusion is a half tooth Class III on the Figure 9 Right Buccal photo. We rely upon the agreed orthodontic correction of the right-side bite. The patient commits to 24 hour elastic wear for bite correction on her right side.

Figure 10: Three Months Post Op 3/23/2009
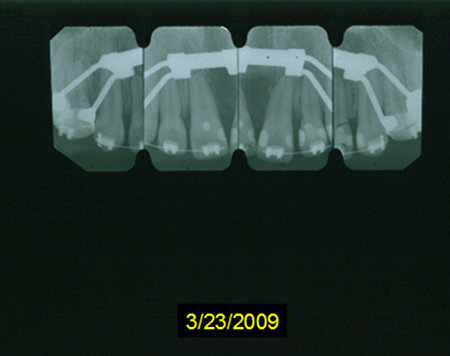
Figure 11: Three Months Post Op 3/23/2009
The repeat of Pano and occlusal views shows the evidence of osteogenesis at the midline of the palate. The Pano described is Figure 10 and the four periapical views are seen at Figure 11 and were all taken on 3/23/2009.

Figure 12: Progress Pano 5/06/2010
Figure 12 shows a Progress Pano taken fourteen months later in treatment during the period of elastics wear and archwire changes. The Pano at this stage of treatment was used to adjust archwires to establish vertical and parallel positions of the teeth.
The root tip rounding associated with two periods of orthodontic fixed appliance tooth movement can be seen throughout the mouth. The closure of the extracted four 1st bicuspids spaces involved major root movement of the teeth adjacent to the extractions.
The root tip rounding associated with two periods of orthodontic fixed appliance tooth movement can be seen throughout the mouth. The closure of the extracted four 1st bicuspids spaces involved major root movement of the teeth adjacent to the extractions.

Figure 13: Pre-removal Photo 10/25/2010
The two periapical views below from the general dentist taken 3-27-09 and 6-18-09 show the eruption of the UL 2nd molar into the UL 3rd molar crown.

Figure 14: Pre-removal Photo 10/25/2010
|

Figure 15: Pre-removal Photo 10/25/2010
|

Figure 16: 12/15/2010 (Age 24Y, 2M) Final Records
The fixed appliance was removed on 12/14/2010. The removal was 10 days short of two years after the surgical procedure. An upper removable retainer and a lower fixed lingual retainer were placed on the day the facial photo in figure 16 was taken.
Figures 17 through 21 are the photos taken on 12/15/2010 and identified as FINAL RECORDS.
Figures 17 through 21 are the photos taken on 12/15/2010 and identified as FINAL RECORDS.

Figure 17
|

Figure 18
|

Figure 19
|

Figure 20
|

Figure 21
We believe that orthodontic treatment delivered to the highest possible standards gives optimum function, esthetics and stability to our patients. The first two areas of improvement can be seen and evaluated on completion of treatment and the removal of the fixed appliance.
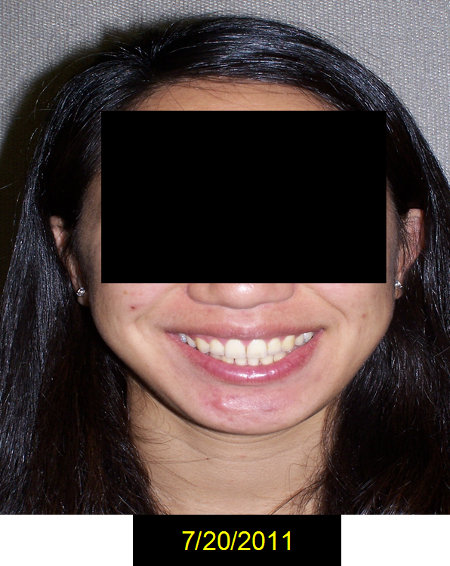
Figure 22
The area of stability is the benefit of orthodontic treatment that can be judged continually and repeatedly as time passes.

Figure 23
The remaining figures show a post final grouping of photos (Figures 22 to 27) taken on 7/20/2011, seven months after appliance removal.

Figure 24
The closing of the spaces occupied previously by the orthodontic bands and the tightening of the bite (for example, the upper right cuspid with the antagonists lower right cuspid and the lower right 2nd bicuspid) are seen on closer examination of the photos.

Figure 25
I wish to thank my staff for the taking of the photos seen in this presentation. I wish to thank our patient for the excellent cooperation and commitment she gave us to obtain this treatment result; an understatement is to say "we could not have done this without her, her records and her professional input."

Figure 26
I especially want to thank Merry Hampton for taking all the radiographs and for her tireless assistance and support. Our office is thankful on a daily basis for her expert aid to us on behalf of our orthodontic patients. Thank you Merry.